


 Alfred Marchal explains the four stages of the wound healing process in plastic surgery and dermatology.
Alfred Marchal explains the four stages of the wound healing process in plastic surgery and dermatology.
After an aesthetic procedure, many factors can interfere with the healing process, thus causing improper or impaired wound healing. The most significant factors that affect cutaneous wound healing and the potential cellular and/or molecular mechanisms are oxygenation1, infection, age and sex hormones, stress, diabetes, obesity, medications, alcoholism, smoking, and nutrition.
There are four stages to the wound healing process — coagulation, inflammation, proliferation, and remodelling2,3.
Step 1: Coagulation
The extravasation of blood into the wound is activated to limit the loss of blood. The clot, comprising of fibrin, fibronectin, vitronectin, Von Willebrand factor, and thrombospondin, provides the provisional matrix for cellular migration.
Step 2: Inflammation
Primary inflammation 24-48 hours
The next wound healing stage is inflammation, with the activation of a classical molecular cascade, which leads to granulocytes or PMNLs (polymorph nuclear leukocytes) infiltrating the wound. These cells are attracted to the wound site within 24 to 48 hours of injury by a number of agents, such as C5a, platelets, TGF-beta, and formyl-methionyl peptide.
Secondary inflammation 48-72 hours
Monocytes are attracted to the wound by a variety of chemo-attractants, including clotting complements, immunoglobulin G (IgG), collagen and elastin, cytokines (such as leukotriene B4), platelet factor IV, PDGF, and TGF-beta.
Macrophages are one of the most important cells present in the later stage of the inflammation process and act as key regulatory cells for repair.
Step 3: Proliferation
Cell proliferation first begins through the migration of fibroblasts, collagen synthesis, and angiogenesis. Next comes granulation tissue formation and, finally, epithelialisation.
Step 4: Remodelling
Matrix synthesis and the remodelling phase are initiated with the development of granulation tissue and continue over prolonged periods of time.
As the matrix matures, fibronectin and hyaluronic acids are broken down. The collagen bundles increase in diameter.
Oxidative stress
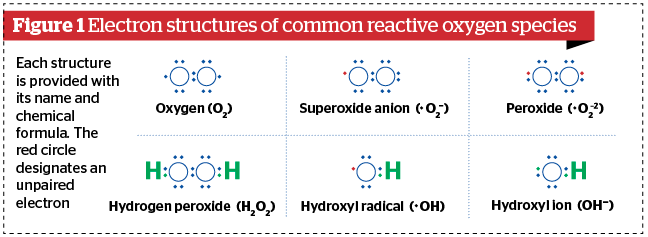
Oxidative stress reflects an imbalance between the systemic manifestation of reactive oxygen species (ROS) and a biological system’s ability to readily detoxify the reactive intermediates or to repair the resulting damage. Disturbances in the normal redox state of cells produce peroxides and free radicals that damage all components of the cell (proteins, lipids, DNA)4.
Oxidative stress from oxidative metabolism causes base damage as well as strand breaks in DNA. Base damage is mostly indirect and caused by the reactive oxygen species (ROS) generated. For example: O2–(superoxide radical), OH (hydroxyl radical) and H2O2 (hydrogen peroxide).
Further, some reactive oxidative species act as cellular messengers in redox signalling. Thus, oxidative stress can cause disruptions in normal mechanisms of cellular signalling.
In humans, oxidative stress is thought to be involved in the development of many diseases and physical effects on the skin. ROS play an important role in skin injury and repair.
Regulation of the wound healing process
The wound-healing process is regulated by a variety of different growth factors, cytokines, and hormones. The innate immune-system cells produce proteolytic and pro-inflammatory enzymes5. They also produce and secrete increased amounts of ROS, required to protect the organism from bacteria and other microorganisms. Additionally, several recent studies revealed that they represent the crucial regulators of this process. Reactive oxygen species are required for the defence against invading pathogens, and at low concentrations, they are the crucial mediators of intracellular signalling. A previous study showed that low H2O2 levels are important for efficient neoangiogenesis in wounds6.
Reactive oxygen species are essential during the healing process at multiple stages, ranging from the initial signal that instigates the immune response to the triggering of intracellular redox-dependent signalling pathways that defend against invading bacteria7,8.
With inflammatory processes, the radical species come largely from neutrophils, eosinophils, and macrophages that release O2, converging in the formation of H2O2.
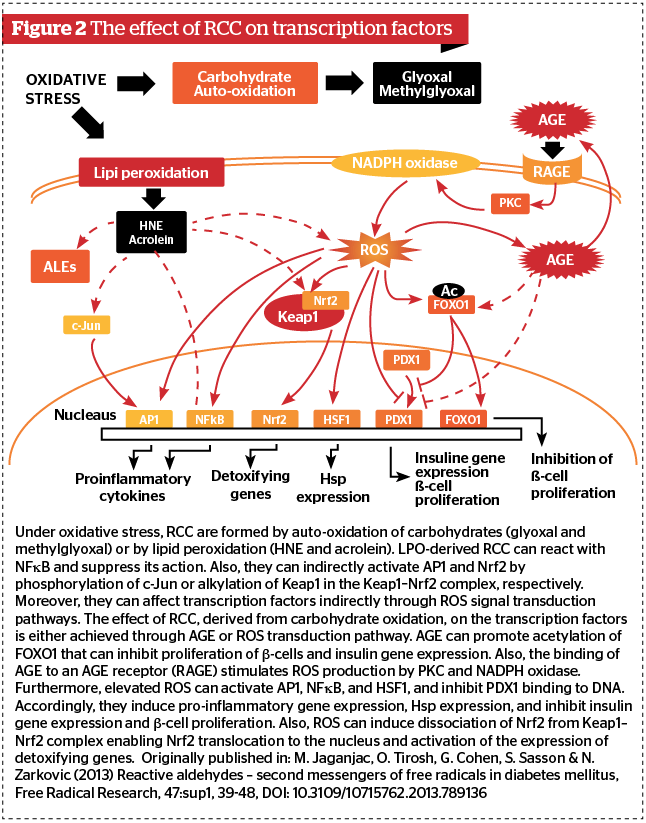
Excessive ROS in the wound environment impedes new tissue formation. Reactive oxygen species are harmful and can cause severe cellular damage. In human and animal cells, the presence of nitric oxide, calcium, and pathogens, can affect the balance between oxidant and antioxidant systems, promoting the generation and accumulation of ROS in cells, eventually inducing oxidative stress9. Oxidative stress can result in DNA damage, mutations, and double-strand aberrations but also induce dysfunction in MAPK/AP-1, NF-κB, and JAK/STAT-signalling pathways, apoptosis, and autophagy10.
Intrinsic and extrinsic factors can lead to skin barrier damage, which leads to the disequilibrium in oxidant and antioxidant balance and induces excessive ROS production.
An aesthetic procedure on the skin will generate varying levels of ROS depending on the size of the wound (surgery as open wounds or superficial as peeling, lasers and burns). A large amount of ROS will generate inflammation, pain, discomfort, and pigmentation after TCA peeling and laser.
Oxidative stress represents the imbalance between oxidative and antioxidative events.
The non-enzymatic antioxidant system includes vitamins C and E, glutathione (GSH), carotenoids, melatonin, A-lipoic acid, Zn (II)-glycine, and polyphenols, and some of these molecules are exogenous antioxidants.
The skin employs a number of endogenous antioxidant agents to protect the oxidative balance, such as superoxide dismutase (SOD), catalase (CAT), glutathione peroxidase (GSH-Px), ascorbic acid, and tocopherols. Results indicate that antioxidant treatments may be effective when applied in the therapy of cutaneous diseases where oxidative stress plays a prominent pathogenic role.
Skin regulates ROS
The antioxidative systems in human skin are interdependent, but they do collaborate. Treatment with known antioxidants, such as ascorbic acid, tocopherols, and polyphenols, increase the resistance of organisms to ROS and prevents skin ageing and inflammation.
An overview of oxidation and skin ageing in clinical practice
Free radicals are unstable chemical species, highly reactive, and formed by the cellular entities of different tissues10. Increased production of these species without any proper effective action by endogenous and exogenous antioxidant systems creates the conditions for oxidative stress.
Antioxidants are chemical substances commonly used in clinical practice for topical application and may contribute to the fight against the radical species responsible for skin damage.
Which antioxidants should you use?
However, for the topical administration of antioxidants to be effective in the prevention and elimination of free radicals it is critical to ensure the stability of the final formulation, since the antioxidant, in most cases, are very unstable and may be oxidised easily, becoming inactive before reaching the site of action. In addition, antioxidants must be properly absorbed through the skin to reach deeper layers of the tissue in the active form.
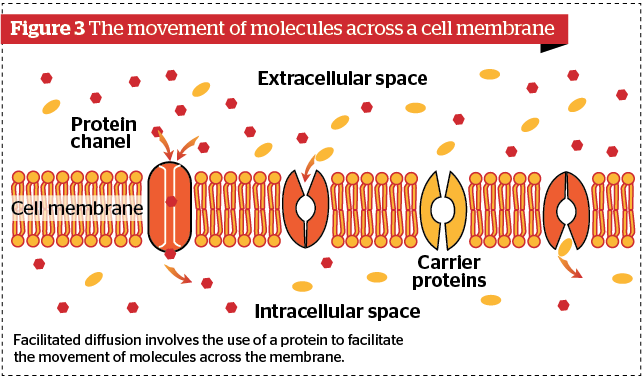
Cell membranes are the main cellular constituents susceptible to oxidation, which is known as lipid peroxidation.
Phenolic compounds are formed in the secondary metabolism of plants and have defence functions. It has been observed that they are capable of reacting with free radicals to form stable chemical species. This power of neutralising the radical structures is due to their chemical structure, which has hydroxyl groups with aromatic rings that confer antioxidant power. The author highlights the flavonoids, phenolic acids, simple phenols, coumarins, tannins, and tocopherols.
The main indications are for superficial aesthetic procedures. For example, it’s very important to use antioxidants before and after peeling, dermabrasion, lasers, microneedling or mesotherapy.
Most compounds must be integrated into modern serums as vectors. We can use polyphenols, tannic acid, vitamin C, glutamine, phytic acid, ginkgo biloba, phytoestrogen, EGCG and curcumin.
Declaration of interest Alfred Marchal is owner of Andromeda Laboratories, board member of Alphascience and initiator in Oncoderma project.
Figures 1, 3 ©; 2 © M. Jaganjac, O. Tirosh, G. Cohen, S. Sasson & N. Zarkovic, Published by Taylor & Francis.
Opening image ©Shutterstock
References:
- David E. Eisenbud. Oxygen in Wound Healing Nutrient, Antibiotic, Signaling Molecule, and Therapeutic Agent. Clin Plast Surg. 2012 Jul;39(3):293-310
- Heather L. Orsted. (2019). Basic Principles of Wound Healing. Wound Care Canada / Volume 9, Number 2
- Dai, T., Tanaka, M., Huang, Y., & Hamblin, M. (2017). Chitosan preparations for wounds and burns: antimicrobial and wound-healing effects.
- Silas Arandas Monteiro e Silva, Gislaine Ricci Leonardi, & Bozena Michniak-Kohn. (2015). An overview about oxidation in clinical practice of skin aging. An Bras Dermatol. 2017 May-Jun; 92(3): 367–374
- Toshihiro Kurahashi, & Junichi Fujii. (2015). Roles of Antioxidative Enzymes in Wound Healing. J. Dev. Biol. 2015, 3, 57-70
- Zhu G., Wang Q, Lu S., & Niu Y. (2017). Hydrogen Peroxide: A Potential Wound Therapeutic Target. Med Princ Pract. 2017;26(4):301-308
- Nicholas Bryan, Helen Ahswin, Neil Smart, & Yves Bayon. Reactive oxygen species (ros) – a family of fate deciding molecules pivotal in constructive inflammation and wound healing. Eur Cell Mater. 2012 Sep 24;24:249-65
- Dunnill, C., Patton, T., Brennan, J., Barrett, J., Dryden, M., & Cooke, J. et al. (2015). Reactive oxygen species (ROS) and wound healing: the functional role of ROS and emerging ROS-modulating technologies for augmentation of the healing process. Int Wound J. 2017 Feb;14(1):89-96
- Xue, J., Yu, C., Sheng, W., Zhu, W., Luo, J., & Zhang, Q. et al. (2017). The Nrf2/GCH1/BH4 Axis Ameliorates Radiation-Induced Skin Injury by Modulating the ROS Cascade. J Invest Dermatol. 2017 Oct;137(10):2059-2068
- Xu, H., Zheng, Y., Liu, Q., Liu, L., Luo, F., & Zhou, H. et al. (2017). Reactive Oxygen Species in Skin Repair, Regeneration, Aging, and Inflammation. DOI: 10.5772/intechopen.72747
- Kohen, R. (1999). Skin antioxidants: Their role in aging and in oxidative stress — New approaches for their evaluation. Biomed Pharmacother. 1999 May;53(4):181-92




{kind=link}