



Jesper Thulesen explains why some patients request the Asian blepharoplasty or double eyelid procedure, the techniques available and the results

Jesper Thulesen, MD, PhD, Dr. Med. Sci., FEBO
is an Oculoplastic Surgeon at Hovedstadens Eye Clinic
(www.eye5.dk), and an Aesthetic Medical Physician at Clinic Aesthetica Kongens Nytorv
(www.clinicaesthetica.dk).
Store Kongensgade 36, 4., 1264 Copenhagen K, Denmark,
email: [email protected]
Asian blepharoplasty, commonly termed double-eyelid surgery, refers to surgery designed to place a crease in Asian eyes that do not have a supratarsal fold in the skin. Patients typically desire to look more bright-eyed and want to make applying eye makeup easier. Patients also seek to remove the puffy and tired look associated with a fatty upper lid and may wish to have a crease similar in appearance to Asian friends who were born with such a crease. Asian patients may also seek to westernise their appearance, although this is controversial.
In the eyelids of the caucasian, the eyelid crease is determined by the insertion of tissue extensions from the deeper connective tissue of the levator aponeurosis to the skin1. The eyelid crease and fold are important aesthetic landmarks and are a vital feature of the upper eyelid appearance. The Asian eyelid has more fullness of the upper eyelid, no crease (‘monolid’) or lower‑lid crease on one or both sides, and narrow palpebral fissures (‘smaller eyes’)2.
History
The earliest reference to upper lid fold creation appears in Japanese literature in the late 1800s3. The surgeon created a fold in the second eye of a female patient born with a fold in only one eyelid. In English literature, the first surgical case was described in the early 1950s4,5. The hallmark of the modern double eyelid operation and probably the most common technique of incisional double eyelid surgery was described in 19606.
Frequency
Approximately 50% of people of Pacific Asian descent (e.g., Korean, Japanese, Chinese) have an eyelid crease — either one or on both sides (Figure 1). The fold represents the insertion of profound tissue fibre expansions from the levator aponeurosis into the dermis (deep skin layer)1. Presumably, Asians have a lower insertion point than in the Caucasian eyelid, leading to smaller or absent folds.
The lower height of the sling in Asians allows the fat to sit lower in the eyelid, leading to a smaller fold. In Asians with a fold, the height of the normal lid fold lies 6–8 mm from the lash line with the skin gently stretched. From the nose, it begins close to the lash line and then reaches a maximum height at the mid pupil. It stays at this height, extending to the bone rim at the side. In contrast, folds in non-Asians tend to be larger due to the height (8–12 mm) and have less fat or fat pads located higher upward than Asians2.
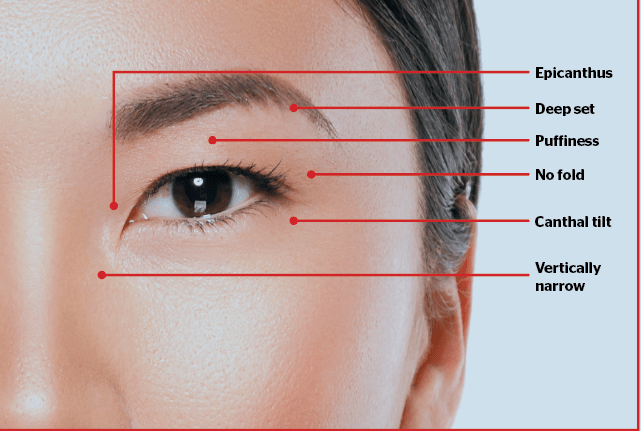
Figure 1 Characteristics of the Asian eye surroundings
Patients
Traditional approaches to placing a crease involve suturing the dermis to a more profound plate of connective tissue in the eyelid — either the so-called aponeurosis or the tarsal plate. Most commonly, the patient for this procedure is female and presents in mid-adolescence or is female and is in her early 20s. Male patients, seen occasionally, tend to be slightly older, aged in their late 20s to early 30s.
Female patients may report difficulty applying eyeliner. Not infrequently, females may apply cellophane tape to create a fold as part of the daily makeup ritual; the patient desires surgery to spare herself this inconvenience (Figure 2). Occasionally, an older patient presents to report problems related to the ageing upper eyelid and/or periorbital area.
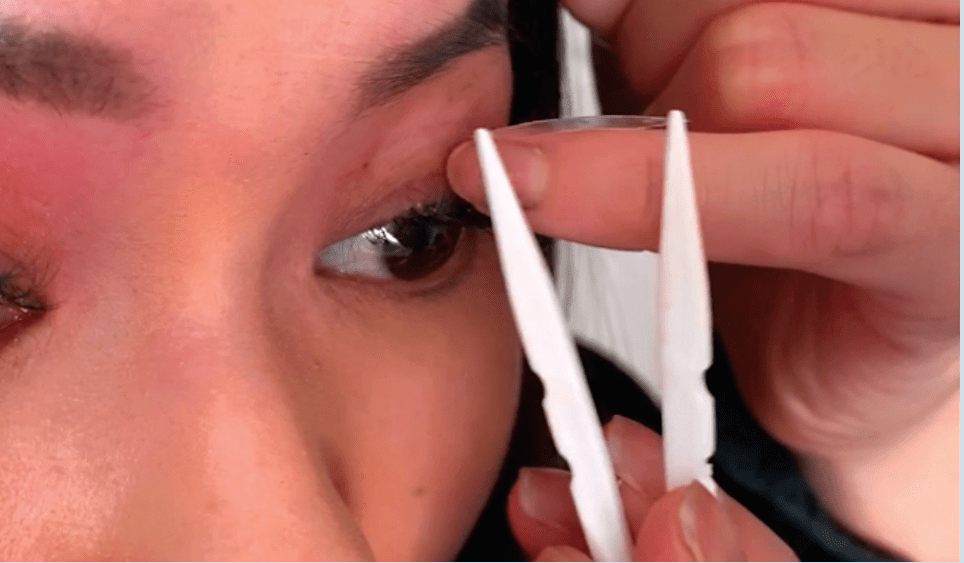
Figure 2 Applying eyelid tape for a temporary shift from the monolid to the double
eyelid appearance
Procedures
The surgical strategy for creating an Asian eyelid fold is either to recreate the skin attachment to the more profound connective tissue plate or to prevent the fat from descending below the desired eyelid fold height. The non-incision suture method (‘closed’ method) of eyelid surgery creates the fold by recreating this skin attachment using transpalpebral stitches to pinch, or invaginate the eyelid skin into a visible crease. The incisional or ‘open’ method of Asian eyelid surgery recreates the fold by removing the inferior portion of the eyelid fat and sealing off this area. A hybrid version, the ‘semi-open’ method, combines aspects of both techniques by using buried stitches to recreate the fold but also removing a portion of the lid fat through a small incision. If the patient wants a more westernised appearance, the surgeon should remove more fat than the standard procedure requires. The height of the proposed crease is determined by using a height of 7–10 mm from the lid margin.
The nasal area of the fold bears a variable relationship to the nasal epicanthal fold. A fold may begin on the undersurface of the epicanthal fold or on the visible outer surface. Reduction of the nasal epicanthal fold is called epicanthoplasty and is often combined with eyelid procedures2.
Contraindications
Patients under eighteen years of age or inadequate maturity.
Surgical Therapy
The two general categories of repair include the ‘closed’ suture method and the ‘open’ incisional method. The closed method is preferable for patients with thin skin (and fat) or Asian eyelids so thin that they fold spontaneously on an intermittent basis. If the patient has some excess fat, this fat can be removed through a small stab incision. The open technique is preferred for patients with thicker skin, thick muscle, or excess skin. Usually, the open incisional technique (‘globe line’) leads to long-term outcome2.
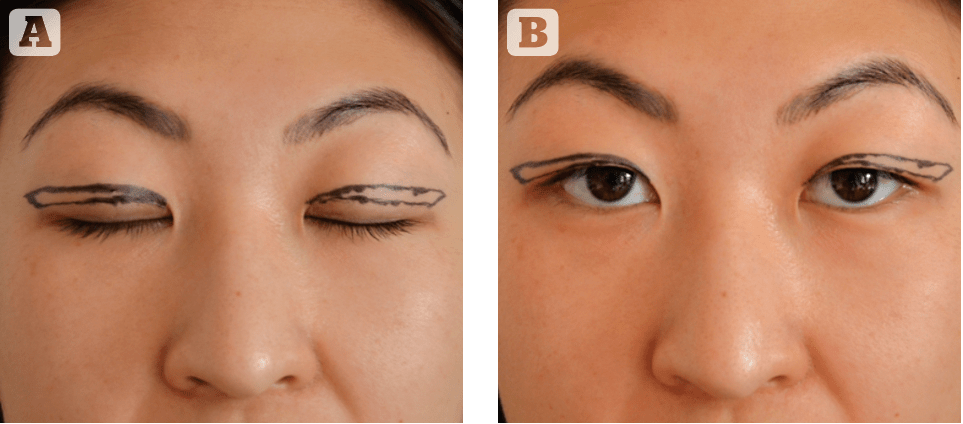
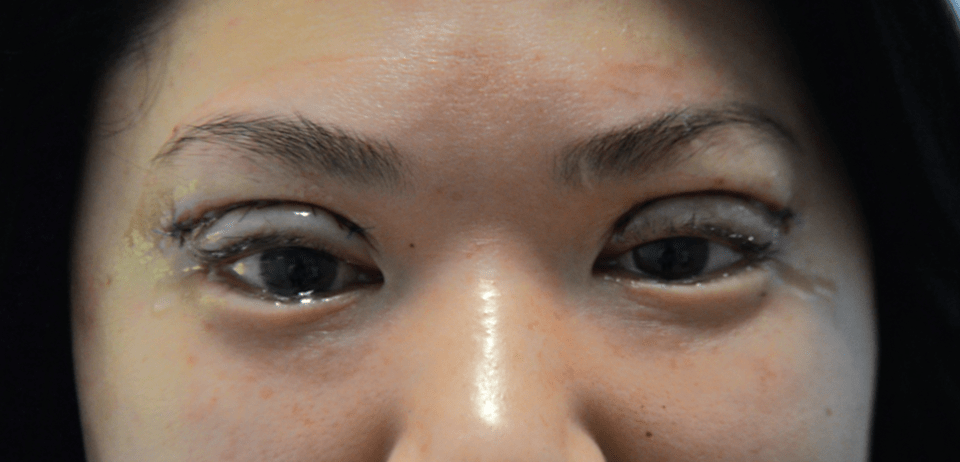
Figure 3 Preoperative assessment for open incisional double eyelid blepharoplasty
Details to focus on before surgery
At pre-examination before surgery, the surgeon considers the upper eyelid position in conjunction with the forehead and the periorbital area (area around the eyes). The visible amount of skin or ‘globe line’, if any, on straightforward gaze depends on the degree of brow ptosis (eyebrows in low position) and upper lid skin redundancy. Even young patients may have a congenitally low brow position.
For a natural-looking fold, the ideal amount of globe line, shown with the eyes open and at straight gaze, is 2-3 mm, and the rest of the skin should be hidden behind the overhanging upper lid skin. The surgeon should be aware that a patient with brow ptosis should have the incision set slightly higher because the brow drops in the postoperative period, decreasing the amount of globe line shown. Most patients have some degree of brow asymmetry, with most patients having a right brow lower than the left. This asymmetry should be compensated for by setting the crease slightly higher or removing slightly more skin from the side with the lower eyebrow. Failure to compensate for the asymmetric brow is one of the frequent causes of crease asymmetry.
Most patients have some minor degrees of asymmetry of the lid margin. The measurement of the so-called marginal reflex distance (MRD) determines those patients who have true ptosis (weakness of the muscle that lifts the upper eyelid), and they should be treated accordingly (for correction of their ptosis). Moderately severe cases of ptosis may need to be treated first, with double-eyelid surgery as a second-stage procedure.
The medial epicanthal area should be addressed in discussion with the patient. If the patient has no preference, the author generally prefers to avoid an epicanthoplasty unless the epicanthal fold is very marked. The patient often makes his or her preference clear on this matter, which of course, influences the size of the fold the surgeon needs to create in order to accomplish the desired result.
Semi-open suture method
The semi-open method incorporates the natural appearance and low morbidity of the closed suture method with the permanence associated with the open method. The lower portion of the eyelid fat is removed through a small incision. This procedure is best suited for younger patients with little forehead ptosis (e.g. high brows) and no prior crease surgery. The upper eyelid skin should be relatively thin, with thin muscle incorporated. The most irreversible deformity that can occur with Asian eyelid surgery is the resection of too much fat. The open suture or semi-open method precludes this complication. The steps of the operation are as follows:
- The eyelids are marked
- After administering intravenous or oral sedation, local anaesthesia is administered beneath the eyelid skin
- After allowing the local anaesthetic to take effect, a 1-cm incision is made. A small sliver of muscle is resected and then small volumes of fat
- Next, four sutures equidistant to each other through the full thickness of the eyelid are placed
- The skin is then closed and a light compression dressing is applied.
- Open incisional method
The preferred height of the incision has already been determined with the patient in the upright position, taking into account the patient’s forehead anatomy. Skin markings are then made (Figure 3). The height is set at the mid pupil, with the rest of the marking continuing at the same height to the side until reaching the bone rim to the temporal side. Toward the nose, the marking tapers smaller toward the caruncle but stops approximately 2–3 mm above the lash line.
An incision is made with a knife or CO2 laser, and the skin can be excised— the amount depends on the degree of preoperative skin excess. A sliver of muscle is removed. Gentle pressure on the globe helps verify the presence of eyelid fat.
Fat can be excised through the septum, and then 6–9 equidistant sutures are placed between the skin and the deep connective plate in the lid in order to make the fold for the globe line. Skin closure is performed using running sutures as in traditional blepharoplasty.
After surgery
Eye ointment is administered, and a light cooling compression dressing is applied. The patient is instructed on the use of eye drops and eye ointment. The surface sutures are removed two weeks postoperatively (Figure 4).
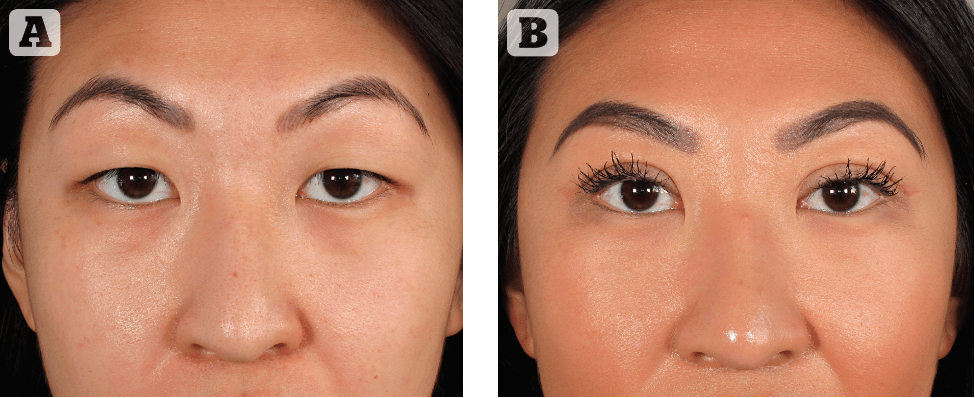
Figure 5 (A) Pre- and (B) postoperative photos. The patient (Chinese origin) underwent
open incisional double eyelid bleferoplasty. Result: High crease with semilunar shape
Complications
Asymmetry
One of the most common causes of asymmetry is unrecognised ptosis (hanging lid due to weak muscle) before surgical procedure. A careful examination is needed to preclude this potential complication.
Another common cause of postoperative asymmetry is the failure to compensate for the asymmetric brow. Most people have one brow lower than the other; in most cases, the right brow is lower. The two creases should compensate for the asymmetry by removing additional upper lid skin from the lower brow. Alternatively, the crease can be set slightly higher on the side with the lower brow. A technical point that contributes to asymmetry is intraoperative swelling that distorts the anatomy.
Reoperation to correct asymmetry is usually performed after 3–8 months.
Loss of crease
The most common cause of crease loss or indistinct crease in either the closed or open method is unrecognised pre-existing ptosis. This is due to the ptotic patient’s dependence on brow lifting in order to open the eyes. In the ptotic eye, the under-functioning muscle is unable to form a complete crease. There are other causes of fold failure. In the closed technique, a common cause is the cheese-wiring effect of the suture through the deeper soft tissues, leading to loss of crease.
In the open technique, another common cause of fold failure is the lack of adequate fixation between the skin and the underlying structures2.
Conclusions
The semi-open and closed methods have many benefits; they possess a relative simplicity and potential reversibility. Scars are less noticeable. Although less permanent than an open procedure, its flexibility makes it a good option for young patients with no previous eye surgery.
The open method is preferred for patients with thicker skin or thick muscle. The procedure is ideal, especially due to the long (often lifelong) durability of the result, together with the option to remove excess skin in the same procedure (Figure 5–6).
Declaration of interest None
Figures 2-6 © Jesper Thulesen
References
- Collin JR, Beard C, Wood I. Experimental and clinical data on the insertion of the levator palpebrae superioris muscle. Am J Ophthalmol. 1978;85:792–801
- Chen WPD. Asian Blepharoplasty and the Eyelid Crease. 3rd. Edition. Elsevier Science, 2016
- Mikano K. A technique in the double eyelid operation. J Chugaishinpo 1896
- Millard DR jr. Oriental peregrinations.Plast Reconstr Surg 1955,16:319-36
- Sayoc BT. Plastic reconstruction of the superior fold in slit eyes. Bull Phil Ophthal Otolaryngol 1953;1:2
- Fernandez LR. Double eyelid operation in the Oriental in Hawaii. Plast Reconstr Surg 1960;25:257-264




{kind=link}