



Grasiela Cássia Monteiro evaluates the changing requirements and treatment strategies when searching for the ideal chin in male and female patients

Professor of Cosmetic Dermatology at Ambulatory of Sanitary Dermatology–Porto Alegre (RS), Brazil
email: [email protected]
A beautiful face, in general, requires harmonious proportions of the facial horizontal thirds and vertical fifths. The chin is of great importance for a beautiful face in both male and female patients. Abnormal proportions between the chin, nose, and the rest of the face are features for the diagnosis of short or long face patterns and micrognathia. To achieve balance in a short face the chin should be elongated, for example, and in a recessed chin, it should be projected. In mild and moderate cases of a recessed chin, injectable fillers can be used, such as hyaluronic acid, calcium hydroxyapatite, and a new option with both substances in the same syringe is also available on the market. Chin deformities are the most common bony abnormality in the face1 and the majority can be treated with fillers. Fillers to the chin can be used for beautification and/or rejuvenation.
Grasiela Cássia Monteiro, MD, MSc,
Professor of Cosmetic Dermatology at Ambulatory of Sanitary Dermatology–Porto Alegre (RS), Brazil
email: [email protected]
In the face, the ageing process leads to skin atrophy, the redistribution of subcutaneous fat, and bone remodelling and resorption. In the lower face, the mandible undergoes anterior and inferior resorption, which the loss of teeth can worsen. The chin becomes more anterior and shorter with ageing2, resulting in loss of jawline definition and facial contour, and modifies the facial proportions. The ageing process modifies all layers of the facial soft tissue as well as the skeleton3.

Anatomy of the chin
Bone
The main structural component is the mandible in the sagittal midline and the mandibular symphysis. Other points include:
- Menton (Me): lowest point on the contour of the mandibular symphysis
- Gnathion (Gn): most anteroinferior point along the contour of the mandibular symphysis
- Pogonion (Pg): most anterior point along the contour of the mandibular symphysis.
Soft tissues
Anterior to the labiomandibular sulcus, from superficial to deep, there is skin, subcutaneous fat, muscles of facial expression (depressor anguli oris, platysma, depressor labia inferioris, and mentalis), deep labiomandibular fat, and deep mental fat in the chin, and periosteum. The inferior margin of the labiomandibular sulcus is formed by the mandibular ligament, anterior to the jowls4.
Inferior to the chin, there are insertions of the muscles platysma, genioglossus, and geniohyoid1.
Vasculature
The primary blood supply to the chin are the mental arteries, which exit the mental foramen on the lateral chin, in line with the vertical axis of the second inferior premolar teeth5. The mental veins also exit from the mental foramen. The mental arteries are terminal branches of the inferior alveolar arteries, which are branches of the maxillary artery. The inferior labial artery and labiomental artery provide further blood supply to the region. The submental artery is a cervical branch of the facial artery. It runs from the exit of the submandibular gland over the mylohyoid and crosses the mandible near the mandibular symphysis2.
Nerves
The mental nerve, a branch of the trigeminal nerve, exits the mental foramen and provides sensory innervation. In the lower face, the motor innervation is given by the branches of the facial nerve, the buccal and marginal mandibular nerves.
Chin assessment
The chin is of great importance for facial attractiveness in men and also in women. The injector should identify chin projection, length and width, dental occlusion, and nasal relationship. It is essential to analyze the labiomental sulcus, mandible angle, pre-jowl sulcus, and cervicomental angle.
The chin should be assessed via horizontal, vertical, and oblique measurements. It is important to identify facial patterns and ascertain whether facial width and length are balanced or whether the patient can be classed as either dolichofacial (long face) or brachyfacial (short face). The subjective facial analysis includes the relationship between maxillae and mandible and the dental occlusion. It is also important to diagnose if the patient is orthognathic, prognathic, or retrognathic. On average, the prognathic profile is more acceptable in men, whereas the retrognathic is preferable in women5.
Rickett’s E-line (a line between the nose tip to the pogonion) assesses the overall alignment of the nose, lip, and chin. The Rickett’s E-line serves as a reference for the protrusion of the lips and should fall 4 and 2 mm from the upper and lower lips, respectively. This line is necessary to identify a malpositioned chin1. Besides that, the true vertical line (TVL) is also important to analyze the chin position in the profile. This TLV is a vertical line dropped to the subnasal point and perpendicular to the Frankfort horizontal plane (FH). The TLV is used to verify the chin position concerning the pogonion point and its projection of the TLV6.
A straightforward way to diagnose micrognathia is to evaluate the measurements of the mandibular arch with the maxillary arch, while if diagnosing retrognathia, one needs to look to evaluate the alveolar overjet. Both micrognathia and retrognathia involve abnormal, arrested development of the mandible. Although it is difficult to distinguish between these conditions, micrognathia refers to the size of the mandible, whereas retrognathia refers to the posterior mandibular positioning in relation to the maxilla7. The Jaw Index can be used to identify micrognathia and it is defined by = Aleveolar overjet x (Maxillary arch/Mandibular arch) in millimetres. The Jaw index measures the maxillary-mandibular discrepancy by quantifying the micrognathic and retrognathic jaw through its alveolar relationship with the maxillary development7.
In general, the mental index (MI) is higher in men than in women; it is measured by the superior border of the foramen mental and the lower mandibular border. In men, the mean of MI was 3.50, while in women, it was 2.968.
It is crucial to identify skeletal abnormalities in the chin as well as soft tissue characteristics.
A system of chin deformities classification was developed by Guyuron and included1:
- Class I: macrogenia— horizontal, vertical, or a combination of both
- Class II: microgenia — horizontal, vertical, or a combination of both
- Class III: combined — horizontal macrogenia with vertical microgenia or horizontal microgenia with vertical macrogenia
- Class IV: asymmetric chin
- Class V: chin-soft tissue ptosis
- Class VI: pseudomacrogenia (normal bony volume with excessive soft tissue)
- Class VII: pseudomicrogenia (normal bony volume with retrogenia secondary to excessive maxillary growth and associated mandibular clockwise autorotation).
In dentoalveolar abnormalities, the injector should consider orthognathic treatment and consider surgical therapy, such as genioplasty and alloplastic chin implants, in severe cases of chin deformities1.
Bertossi and colleagues in 2015 proposed that microgenia with sagittal chin deficiency less than 4 mm from the true vertical line (or profile line, a vertical line in the subnasale perpendicular to the Frankfort horizontal plane) or with mild asymmetry, with normal soft-tissue chin thickness (mean 8–10 mm) can be treated with injectable fillers. Furthermore, patients aged over 50 years affected by sagittal chin deficiency of more than 4 mm with a reduction of soft-tissue chin thickness (mean 6.5 mm) have been corrected with the use of fillers6.
Treatment planning
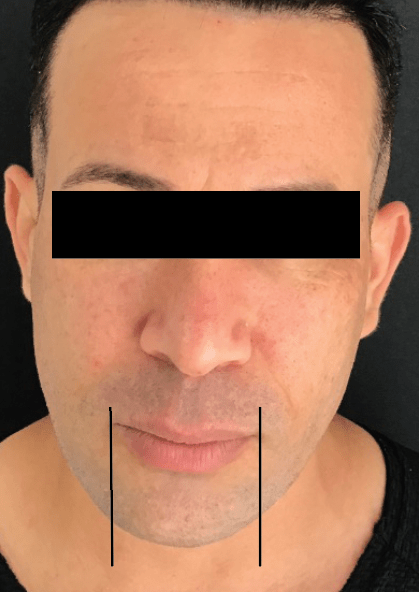
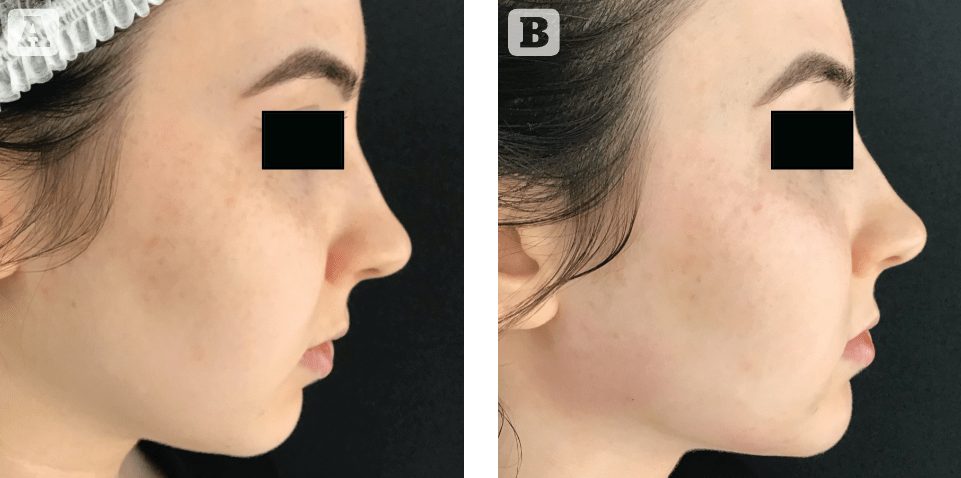
In the male patient, the ideal width of the chin is equal to the width of the mouth, and the ideal projection is approximately as far as the lower lip. Whereas in the female patient, the ideal width of the chin is equivalent to the medial intercanthal distance and in women, the lower lip should be 1 to 2 mm beyond the chin2 (Figures 1–2). Besides that, the lower face in men is, in general, marked by a sharper and more defined jawline and a wider and larger chin area9, 10. The female chin is more pointed and rounded. If the bellies of mentalis muscle are visible in a woman, consider filler to create a more feminine appearance. To mark the chin area, the injector should mark a semicircle in the mental area respecting the intercanthal or the mouth width according to the desired female or male chin. The inferior border of this semicircle is the mandible bone and the superior is the labiomental sulcus. To treat the chin area, the injector should choose fillers with very high G prime with hyaluronic acid, calcium hydroxyapatite, or both products in the same syringe. If the injector prefers a needle, it is necessary to touch the bone in the supraperiosteal plane and aspirate before injecting to avoid any vascular occlusion. The author recommends the use of 22 or 23 G 40- or 50 mm cannulas to treat the chin. A tip to treat the chin in men with cannula is the use of a manoeuvre which we call Braz-Monteiro (described with Dr. André Braz in the scientific literature). This manoeuvre was created because the mentalis muscles in males are stronger and have more muscle mass than in females making it difficult to use the cannula. Outside the semicircle, we use an injection point of lidocaine to anaesthetise and relax the mentalis muscles. Using the entry point, we introduce the cannula, pinching the mentalis muscle with the non-dominant hand and displacing anteriorly and superiorly, creating a space behind the mentalis muscles. The technique is retroinjection with 80% of the total amount in the supraperiosteal plane and 20% of it in the subcutaneous. The amount to use in each session is 0.5–1.0 cc. Many sessions can be performed. To restore or create an anterior projection to the chin, the filler should be placed in the pogonion and submuscular below the mentalis muscles. If the injector wishes to augment the length of the chin, the filler should be placed in the submental area.
Conclusion
The use of filler treatments in the chin area while respecting gender differences is a suitable option for recessed cases, correction of small defects, and asymmetries. More severe cases should be managed with surgery and genioplasty, especially when the patient presents with respiratory difficulties. Injectors can use a cannula to place filler in the chin area in both female and male patients in an easy method with the Braz-Monteiro manoeuvre.
Declaration of interest None
Figures 1-3 © Grasiela Cássia Monteiro
References
- Ward J, Podda S, Garri JI, Wolfe SA, Thaller SR. Chin deformities. J Craniofac Surg. 2007;18(4):887-94.
- Braz A, Eduardo CCP. Reshaping the Lower Face Using Injectable Fillers. Indian J Plast Surg. 2020;53(2):207-18.
- Wong CH, Mendelson B. Newer Understanding of Specific Anatomic Targets in the Aging Face as Applied to Injectables: Aging Changes in the Craniofacial Skeleton and Facial Ligaments. Plast Reconstr Surg. 2015;136(5 Suppl):44s-8s.
- Vazirnia A, Braz A, Fabi SG. Nonsurgical jawline rejuvenation using injectable fillers. J Cosmet Dermatol. 2020;19(8):1940-7.
- Braz A, Sakuma T. Atlas de Anatomia e Preenchimento Global da Face. 1 edição ed. Rio de Janeiro,Brazil: Guanabara Koogan; 2019.
- Bertossi D, Galzignato PF, Albanese M, Botti C, Botti G, Nocini PF. Chin Microgenia: A Clinical Comparative Study. Aesthetic Plast Surg. 2015;39(5):651-8.
- Mermans JF, Ghasemi SM, Lissenberg-Witte BI, Don Griot JPW. The Reproducibility of the Jaw Index in the Measurement of Healthy Newborns. Cleft Palate Craniofac J. 2020;57(5):574-80.
- Sghaireen MG, Alam MK, Patil SR, Rahman SA, Alhabib S, Lynch CD, et al. Morphometric analysis of panoramic mandibular index, mental index, and antegonial index. J Int Med Res. 2020;48(3):300060520912138.
- Rossi AM, Fitzgerald R, Humphrey S. Facial Soft Tissue Augmentation in Males: An Anatomical and Practical Approach. Dermatol Surg. 2017;43 Suppl 2:S131-s9.
- Braz A, Eduardo CCP. The Facial Shapes in Planning the Treatment with Injectable Fillers. Indian J Plast Surg. 2020;53(2):230-43.





{kind=link}