



Ibrahim A. Ashary and Mawada N.Barakia share the results of a
retrospective study on 120 patients undergoing rhinoplasty using the
Ashary Sandwich technique

Consultant plastic surgeon, Greifswald University; Germany; Mawada N.Barakia, B.D.S. University of Medical Sciences and Technology; Khartoum, Sudan
email [email protected]
Concavity of the lateral crus is often a difficult problem to address both aesthetically and functionally1. Flaccid lower lateral cartilages (LLC) cause the concavity of the nasal sidewall. These depressions produce not only a cosmetic deformity but additionally cause airway obstruction by protruding downward into the nasal vestibule, inflicting external valve pathology, which is principally seen once the whole lateral crura become concave2.
For the above reasons, the position of the lower lateral cartilages was found to be closely associated with the function of the external nasal valve (ENV)3.
Lower lateral cartilage concavities can exist secondary to inherent asymmetries, structural weaknesses of crura, or complete absence of the lateral crura, leading to a pinched tip. The normal anatomy of the distal nose may be a reflection of fine integration between the lower lateral cartilage, the upper lateral cartilage, the septum, and skin. Understanding these relationships can allow the operating surgeon to diagnose and treat concavities of the distal nose.
The area of concavity and the functional impairment dictates the correction. Once a unilateral irregularity exists in the lower lateral cartilage, the tripod length is affected, inflicting not only the topographic concavity but additionally a deviation of the nasal tip to the aspect of the shorter lateral crus.
The lateral crura should be convex at the nasal dome with gradual flattening toward the pyriform aperture4.
Anatomically this cartilage was found to possess a three-dimensional hemispheric look and is connected to the upper lateral cartilage (ULC) at the scroll space by an inward limb. This inward limb might have a crucial role in producing asymmetry and flare of the anterior naris. At least one-third of the LLC analyzed had a medial wall in addition to the lateral wall, that remarkably increased the flare and recoil force of this structure. This makes this cartilage more redundant to reshaping procedures (straightening). Thus, special attention should sometimes be paid to the common anatomic variation to provide symmetric nostrils and to get an additional aesthetically acceptable alar tip5.
To overcome this drawback, several techniques were introduced and successfully used by many authors1.
Patients and methods
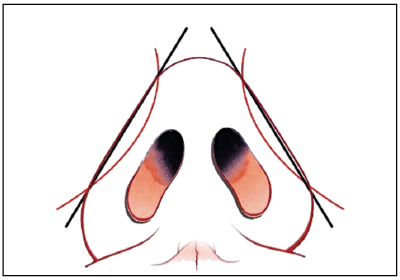
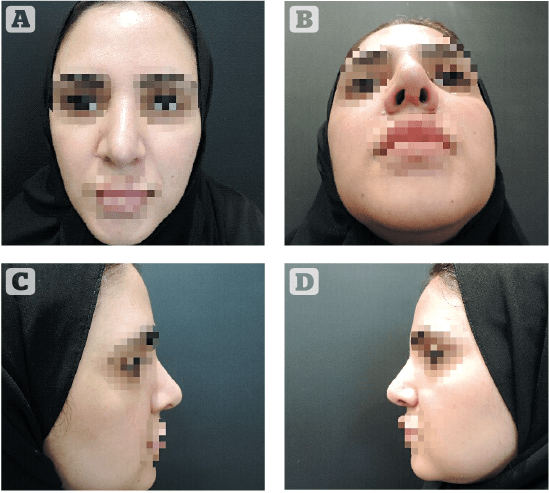
A retrospective study in 120 patients who underwent primary and secondary rhinoplasties from November 2018 to November 2019 to restore lower lateral cartilage concavity (Figure 1) using the Ashary sandwich technique, patients were followed up for 6 months, deformities were analyzed pre- and postoperatively based on clinical evaluation and standardized photographs. Patient satisfaction was evaluated subjectively.
Operative procedure
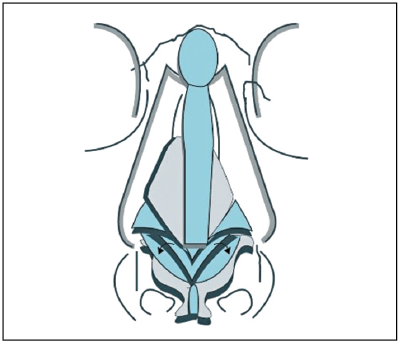
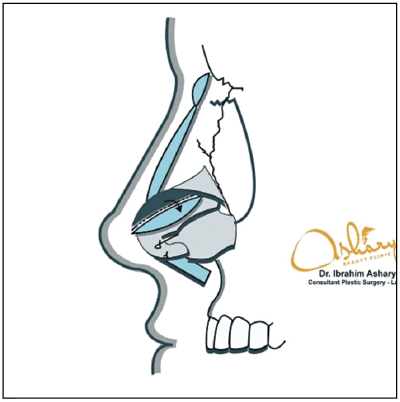
This technique uses an open rhinoplasty approach; additionally, the caudal part of the lower lateral cartilage (LLC) is not removed entirely. It is flipped over and used as a graft for the defected part of the LLC and then sutured (Figures 2,3). The LLC ligament is not removed in order to stabilize the graft, and there is no need for further fixation due to the stable position of the graft. Depending on the defect, the surgeon can decide to perform a unilateral or bi-lateral sandwich technique. In addition, in rare cases such as cleft noses, if the sandwich technique cannot entirely fill the defect, the surgeon can add a graft that is taken from the septum. Moreover, the author advised that vicryl is more efficient in graft fixation due to its non-irritation effect on the skin and it causes less fibrosis on the dermis, which usually affects the result. Most surgeons use prolene because of its non-absorbable nature; however, this suture causes more fibrosis and sometimes infection.
Results
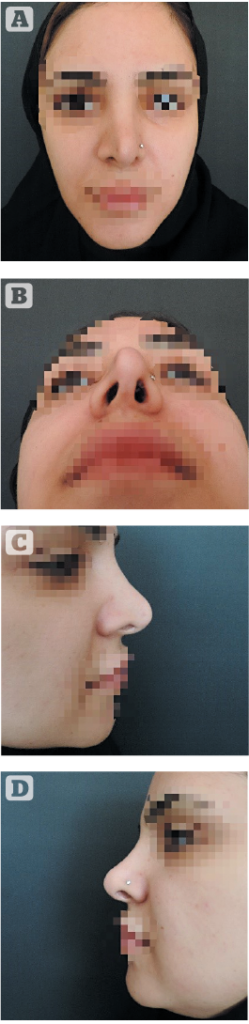
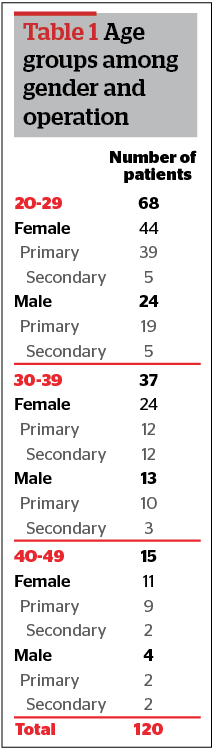
The sandwich technique was performed in 120 rhinoplasties, 41 males and 79 females; 68 of these patients were in the age range of 20 to 29, 37 were in the range of 30 to 39, and 15 were in the range of 40 to 49; 75.83% of the operations were primary rhinoplasties, and 24.16% were secondary (Figure 4a, b, c, d).
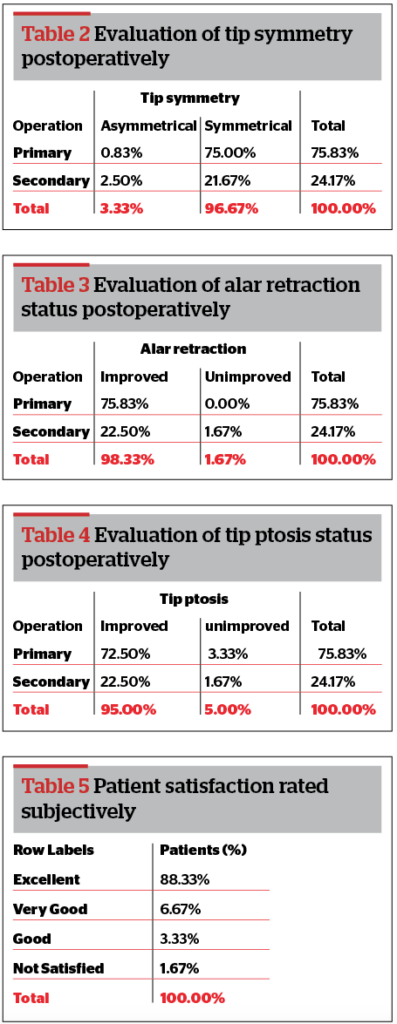
The postoperative results showed a clear improvement in LLC concavity, which reflected on the tip symmetry (96.67%).
Alar retraction was improved in (98.33%), and tip ptosis was improved in (95%).
Results also showed that the function of the external nasal valve and the alar pinch were improved 100% in both primary and secondary rhinoplasties; the average follow-up period was 6 months. Patient satisfaction was evaluated, and patients rated the result as ‘excellent,’ (88.33%), as ‘very good,’ (6.67%) as ‘good,’ (3.33%) and as ‘not satisfied’ (1.67 %) (Figure 5a, b, c, d).
Conclusion
Lower lateral cartilage concavity is frequently followed by dysfunction of the external nasal valve and aesthetic deformities, with the use of the sandwich technique we completely rebuilt the structure of the nasal tripod and therefore the function and aesthetics of the nose. The technique was proven to be effective and efficient.
Declaration of interest None
Figures 1-5 © Dr Ashary
Tables 1-5 © Dr Ashary
REFERENCES
- Tardy ME. Sculpture of the nasal tip. Rhinoplasty: The Art and the Science. 1996; 2
- TerKonda RP, Sykes JM. Repairing the twisted nose. Otolaryngologic Clinics of North America. 1999 Feb 1;32(1):53-64
- Howard BK, Rohrich RJ. Understanding the nasal airway: principles and practice. Plastic and reconstructive surgery. 2002 Mar 1;109(3):1128-46
- Howard BK, Rohrich RJ. Understanding the nasal airway: principles and practice. Plastic and reconstructive surgery. 2002 Mar 1;109(3):1128-46
- Hafezi F, Naghibzadeh B, Nouhi AH. Applied anatomy of the nasal lower lateral cartilage: a new finding. Aesthetic plastic surgery. 2010 Apr 1;34(2):244-8





{kind=link}