

Andrew Campbell, discusses the use of a fractionated hybrid laser for both facial and non-facial skin tightening and wrinkle reduction.
 Historically speaking, there have been very few techniques available to significantly rejuvenate the skin of the body. Facial skin, on the other hand, can be treated with a variety of very aggressive maneuvers to create very significant rejuvenation. Treatments such as phenol based chemical peels, dermabrasion, and aggressive lasers such as the CO2 laser and erbium lasers have all been used for decades to create amazing wrinkle reduction, skin tightening, and overall skin rejuvenation. Unfortunately, these aggressive treatments can not be used on the skin of the body.
Historically speaking, there have been very few techniques available to significantly rejuvenate the skin of the body. Facial skin, on the other hand, can be treated with a variety of very aggressive maneuvers to create very significant rejuvenation. Treatments such as phenol based chemical peels, dermabrasion, and aggressive lasers such as the CO2 laser and erbium lasers have all been used for decades to create amazing wrinkle reduction, skin tightening, and overall skin rejuvenation. Unfortunately, these aggressive treatments can not be used on the skin of the body.
Any treatment of the skin that ablates the full thickness of the epidermis creates the need for the epidermis to resurface itself. This occurs when the epidermis from pilosebaceous units migrates across the remaining exposed dermis to create new epidermal protection. Even though the dermis will take months for all the neocollagenesis to occur, once the epidermis resurfaces, the superficial healing process is complete. On the face, these pilosebaceous units are relatively close to one another so the epidermis can migrate and completely heal within 7–10 days. Unfortunately, on skin of the body the pilosebaceous units are so far apart that it would take well over 14 days to accomplish this healing, a time that is so long as to virtually guarantee the appearance of scar tissue. Therefore, it is impossible to rejuvenate the skin of the body with a full field trans-epidermal injury. This leaves us with lighter chemical peels, such as salicylic acid peels, or non-ablative treatments, such as intense pulsed light. These modalities do not create enough dermal remodeling to significantly improve wrinkles or cause skin tightening.
More recently, fractionated lasers have been created to allow for the injury of the deeper dermal skin while leaving uninjured epidermis around the fractionated injury. This allows for healing to occur across just the fractionated spot, something that can be done in about 5–7 days for most devices. This then allows for the safe improvement of the skin of the body. The only difficulty is that in order to cause a deep enough and significant enough injury, many of these devices, such as fractionated CO2 or fractionated 1550 nm lasers end up causing too much injury, risking complications, or, when used with less power, give less than impressive results.
Hybrid fractional laser
The world’s first hybrid fractional laser (Halo laser by Sciton, Palo Alto, CA) uses a combination of the erbium laser with a 1470 nm laser. This combination or hybrid laser is fractionated and was developed to further reduce downtime and risk while maximizing the effect it has on the dermis in order to cause as much skin rejuvenation and wrinkle reduction as possible. The erbium laser is an erbium doped yttrium-aluminum-garnet laser. The wavelength emitted is 2940 nm. This wavelength is at the peak of the water absorption curve, giving it 11 times the absorption in water compared to the CO2 laser. As an ablative laser, this increased absorption means less heat is deposited into the tissue during a resurfacing procedure since the laser does not penetrate into the skin, but rather vaporizes the skin on contact, leaving very little thermally damaged or necrotic tissue behind. This gives an advantage to the erbium laser in that it can vaporize a very small amount of superficial skin, essentially allowing it to just treat the superficial epidermis, minimizing any risk and recovery. While the erbium laser can be fractionated and used alone, the author believes the deeper treatments create a significant amount of downtime and can occasionally create a waffle pattern on the skin of the body.
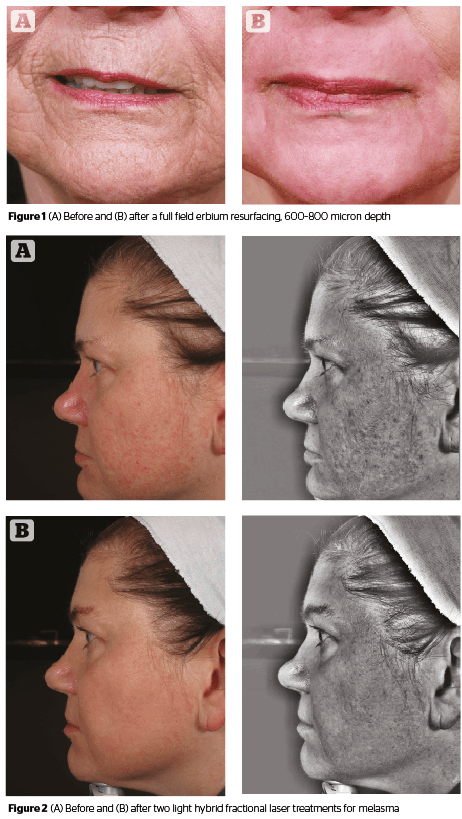
 The 1470 nm laser is used non-ablatively, and can penetrate the skin to a maximum of 700 microns, coagulating the tissue, causing neocollagenesis, and tissue tightening. As can be noted in the treatment parameters for full field deep erbium laser resurfacing, this depth seems to be quite adequate in causing very significant wrinkle reduction (Figure 1). Because the laser causes a non-ablative or coagulative wound, and does not vaporize the tissue, there is typically no weeping or drainage from the skin, and thus the downtime is minimized. The coagulation does cause injury to the epidermis, but the author finds the epidermis is healed and viable within 24 hours of the treatment, thus limiting any risks and downtime. The author has found that the hybrid fractional laser can improve the appearance of the skin better than a fractionated erbium alone. This is impressive considering that the fractionated erbium would cause weeping and downtime for 3–5 days, while the hybrid fractional laser allows patients to wear makeup the next day. Due to the fact that the downtime is minimal in comparison and the results witnessed by the author better, the hybrid fractional laser has replaced the standard fractionated erbium laser in the author’s practice.
The 1470 nm laser is used non-ablatively, and can penetrate the skin to a maximum of 700 microns, coagulating the tissue, causing neocollagenesis, and tissue tightening. As can be noted in the treatment parameters for full field deep erbium laser resurfacing, this depth seems to be quite adequate in causing very significant wrinkle reduction (Figure 1). Because the laser causes a non-ablative or coagulative wound, and does not vaporize the tissue, there is typically no weeping or drainage from the skin, and thus the downtime is minimized. The coagulation does cause injury to the epidermis, but the author finds the epidermis is healed and viable within 24 hours of the treatment, thus limiting any risks and downtime. The author has found that the hybrid fractional laser can improve the appearance of the skin better than a fractionated erbium alone. This is impressive considering that the fractionated erbium would cause weeping and downtime for 3–5 days, while the hybrid fractional laser allows patients to wear makeup the next day. Due to the fact that the downtime is minimal in comparison and the results witnessed by the author better, the hybrid fractional laser has replaced the standard fractionated erbium laser in the author’s practice.
Due to it’s efficient absorption by water, the erbium laser is one of the few lasers that can actually ablate the superficial epidermis without depositing a large amount of heat in the underlying tissue. Since the CO2 laser will penetrate into the skin about 50–100 microns before the energy is completely absorbed, it leaves behind a layer of tissue that has thermal necrosis. This layer can be 50–100 microns thick. This is about the thickness of the epidermis itself, so it’s physically impossible for the CO2 laser to ablate the superficial epidermis without effecting the entire thickness of the epidermis. Additional passes or deeper treatments with a CO2 laser add to the heat in the tissue, effecting it’s ability to heal quickly. The erbium laser, however, only penetrates the epidermis by about 4 microns before being completely absorbed. When the erbium laser vaporizes the superficial epidermis, it leaves behind about 4 microns of thermal necrosis, an amount that really has no consequences. As such, the erbium laser can be used to treat the epidermis itself, without creating the need for the resurfacing of epidermal cells from the pilosebaceous units. In essence, it is just vaporizing the most superficial aspect of the epidermis, while leaving the deeper portions of the epidermis intact and viable. This treatment is called an intra-epidermal peel.
 In the hybrid fractional laser, the erbium laser is used to vaporize a superficial intra-epidermal spot over the non-ablative injury to both help the expression of necrotic debris from the non-ablative injury, and to create a cascade of enzymes that causes neo-collagenesis deep into the dermis1. This neocollagenesis of the dermis occurs through the release of a variety of mediators, including metalloproteinases, due to this superficial epidermal injury. These metalloproteinases ultimately break down some of the dermal collagen, causing the deposition of procollagen and new collagen in the dermis. Together, the erbium laser and 1470 nm laser act synergistically to rejuvenate the skin. One indirectly effects the dermis through mediators, while the other directly coagulates the dermal tissue. Because the erbium injury is so superficial, and the 1470nm laser is non-ablative, there is minimal to no drainage from the skin. Therefore, patients can apply a moisturizer to prevent flaking, and then makeup to camouflage any discolorations. Most patients continue their normal activities starting the day after the procedure.
In the hybrid fractional laser, the erbium laser is used to vaporize a superficial intra-epidermal spot over the non-ablative injury to both help the expression of necrotic debris from the non-ablative injury, and to create a cascade of enzymes that causes neo-collagenesis deep into the dermis1. This neocollagenesis of the dermis occurs through the release of a variety of mediators, including metalloproteinases, due to this superficial epidermal injury. These metalloproteinases ultimately break down some of the dermal collagen, causing the deposition of procollagen and new collagen in the dermis. Together, the erbium laser and 1470 nm laser act synergistically to rejuvenate the skin. One indirectly effects the dermis through mediators, while the other directly coagulates the dermal tissue. Because the erbium injury is so superficial, and the 1470nm laser is non-ablative, there is minimal to no drainage from the skin. Therefore, patients can apply a moisturizer to prevent flaking, and then makeup to camouflage any discolorations. Most patients continue their normal activities starting the day after the procedure.
 The hybrid fractional laser hand piece has a port for the attachment of a Zimmer cooling unit, so cold air is passed across the treated skin to improve comfort. On the opposite side of the hand piece, there is a suction port to evacuate the very small amount of plume that is created by the erbium laser. The hand piece also has an optical tracker so the device can determine the speed at which the hand piece is rolling across the skin. It also has a temperature sensor to determine the surface temperature of the skin. The computer then varies the rate of the individual laser firings as well as the power of each firing depending on the speed of the hand piece and the temperature of the skin. This allows for an extremely precise and consistent treatment.
The hybrid fractional laser hand piece has a port for the attachment of a Zimmer cooling unit, so cold air is passed across the treated skin to improve comfort. On the opposite side of the hand piece, there is a suction port to evacuate the very small amount of plume that is created by the erbium laser. The hand piece also has an optical tracker so the device can determine the speed at which the hand piece is rolling across the skin. It also has a temperature sensor to determine the surface temperature of the skin. The computer then varies the rate of the individual laser firings as well as the power of each firing depending on the speed of the hand piece and the temperature of the skin. This allows for an extremely precise and consistent treatment.
Treatments
A hybrid fractional treatment is performed on the face using topical anesthetic. However, there is very little discomfort when treating non-facial areas, therefore, no anesthetic is required for these treatments. The non-ablative 1470 nm laser and the 2940 nm erbium laser can be independently controlled for depth and density. In order to limit edema and discomfort, most treatments are performed with a depth of 400 microns for the 1470 nm non-ablative laser, though treatments at it’s most aggressive setting of 700 microns can still be easily tolerated with topical anesthetic and the cooling unit. To prevent any minimal drainage from the skin, the erbium laser is usually set to less than 40 microns, most commonly 20 microns. Desired densities can vary by skin condition, but most off face treatments are at 20% coverage for both the non-ablative and ablative lasers. This density allows for the very significant improvement in pigmentation and vascularity of the skin as well as improvement in wrinkles, texture, and skin tightening.
 To perform a treatment, the provider simply wipes the planned treatment area clean with alcohol, then uses the hand piece to track across the width and the length of the subunit being treated. This allows the computer to calculate the surface area of the region. The depth and density of each laser is then adjusted and the treatment begins. The provider simply rolls the hand piece across the skin in the area being treated in a methodical way to assure even distribution of the fractionated injuries. This is continued in different directions until the desired density is achieved at which point the computer will beep, notifying the provider that the treatment is complete. The next region is then treated in an identical fashion until the entire planned treatment is complete. At that time, the skin will feel quite hot, but the cooling unit limits any discomfort. A cooling gel is then applied that dramatically reduces the sensation of heat.
To perform a treatment, the provider simply wipes the planned treatment area clean with alcohol, then uses the hand piece to track across the width and the length of the subunit being treated. This allows the computer to calculate the surface area of the region. The depth and density of each laser is then adjusted and the treatment begins. The provider simply rolls the hand piece across the skin in the area being treated in a methodical way to assure even distribution of the fractionated injuries. This is continued in different directions until the desired density is achieved at which point the computer will beep, notifying the provider that the treatment is complete. The next region is then treated in an identical fashion until the entire planned treatment is complete. At that time, the skin will feel quite hot, but the cooling unit limits any discomfort. A cooling gel is then applied that dramatically reduces the sensation of heat.
Patients usually apply a gel on the treated area the first day of the treatment to help with mild erythema and the hot sensation. The following day, most wear a heavy moisturizer. A mild amount of edema is expected and can be minimized by the use of a medrol dose pack started prior to the treatment. This edema resolves over 3–7 days. For facial treatments, any patient with a history of cold sores is placed on antiviral medication prophylactically. For off-face treatments, the author believes this is unnecessary. Considering the epidermis is fully healed within 24 hours, the use of prophylactic antibiotics and antifungals is not required.
Even though the hybrid laser does not directly target melanin or hemoglobin, the laser can none the less, cause a very significant improvement in browns and reds of the skin through the dermal coagulation of the tissue. This injury allows for the direct coagulation of any vascular structures in that area, reducing the visibility of visible vessels. The coagulation also causes the expulsion of unwanted pigmentation up through the tunnel of injured tissue. The melanin gets trapped in small areas of microscopic epidermal necrotic debris (MENDs) at each spot of laser injury. These MENDs come to the surface of the skin and slough over the first 3–7 days after the treatment. This sloughing can be camouflaged with the moisturizer and mineral makeup. Once the healing is complete, the color of the skin is improved. The wrinkle reduction and improvement in pore visibility and skin tightening will continue to improve over several months.
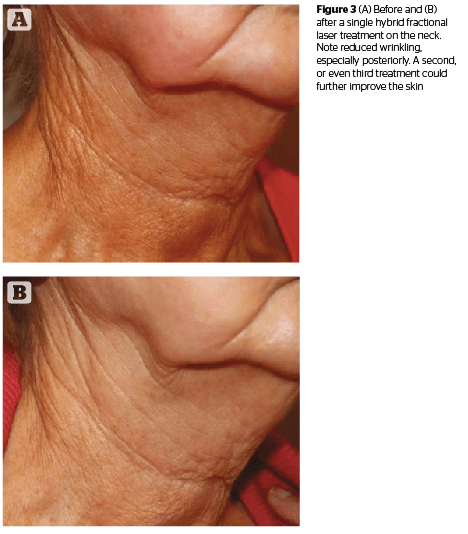
 The combination of the non-ablative injury with the very superficial ablation creates significant skin rejuvenation while minimizing or eliminating any downtime. The risks of any complications are also extremely low and none have been witnessed by the author over several hundred treatments other than some temporary hyperpigmentation after a very aggressive (700 micron) treatment for skin depressions in one patient. The unwanted pigmentation resolved after a second, more typical treatment at 400 microns. Several patients with melasma have been treated with the hybrid fractional laser with significant improvement. These were patients that were already maximized with skin care, 4% hydroquinone, sunblock, and broad band light treatments. They noticed a very good improvement in their remaining pigmentation after hybrid fractional laser treatments (Figure 2).
The combination of the non-ablative injury with the very superficial ablation creates significant skin rejuvenation while minimizing or eliminating any downtime. The risks of any complications are also extremely low and none have been witnessed by the author over several hundred treatments other than some temporary hyperpigmentation after a very aggressive (700 micron) treatment for skin depressions in one patient. The unwanted pigmentation resolved after a second, more typical treatment at 400 microns. Several patients with melasma have been treated with the hybrid fractional laser with significant improvement. These were patients that were already maximized with skin care, 4% hydroquinone, sunblock, and broad band light treatments. They noticed a very good improvement in their remaining pigmentation after hybrid fractional laser treatments (Figure 2).
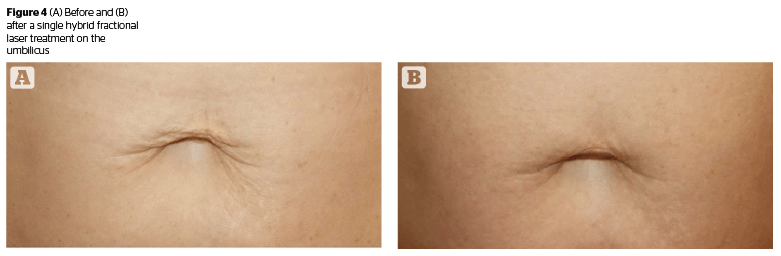
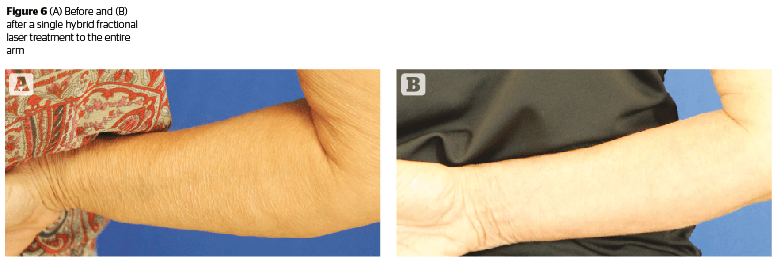
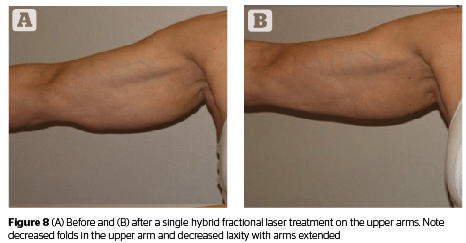
Since the laser is fractionated, it is safe to use off-face. It can be used to treat photo damage and wrinkling of the neck, chest, arms, abdomen, hands, and knees. Darker skin types can also be treated, though skin type VI has not been studied by the author (Figures 3–8).
Conclusion
The hybrid fractional laser is a very versatile tool in aesthetic medicine. It can be used to create very significant improvement in the aesthetic quality of facial and non-facial skin, all while greatly minimizing the risks, complications, side effects, and downtime of more traditional modalities.



