



Midey Mohammad Helmy describes the results of a study on treating gummy smile using botulinum toxin injections

email: [email protected]
Fixing a smile is one of the most popular and sought after procedures in the aesthetic world. It is not only the appearance of a gummy smile that triggers the patient to seek an aesthetic solution, as an unsatisfactory smile can also create difficulty in communication or self-expression for the patient. The ongoing advances in science and technology offer many solutions to most of the problems facing the physician as well as allowing for greater patient satisfaction rates. Also, the patient’s high demands dictate more novel and creative approaches to ensure practitioners provide the best quality of life possible to the patient.
Understanding the complex anatomy of the overlapping muscles of the lower face region is key to determine the exact cause of excessive gingival display, thus allowing for better and more natural-looking results. The muscles functionally involved in raising the upper lip have a role in tooth and gum display during smiling, these include the levator labii superioris alaeque nasalis (LLSAN), levator labii superioris, zygomaticus major (ZM), zygomaticus minor, levator anguli oris (LAO), orbicularis oris, and risorius. A therapeutic approach in which the LLSAN muscle alone is treated with botulinum toxin may be insufficient when other muscles are involved in the excessive gingival display1,2.
There are many reasons that can contribute to the condition of excessive gingival display, the most common being:
- Hyper-active elevator muscles of the upper lip
- Incompetent upper lip
- Skeletal defects (such as maxillary prognathism and maxillary canting)
- Inward inversion of the upper lip
- Short clinical crowns
- Misaligned teeth3–7.
An excessive gingival display may persist after orthodontic treatment or gingivectomy in cases of short clinical crowns. Also, severe gummy smile with class II malocclusion can be treated with LeFort I osteotomy combined with horseshoe osteotomy and intraoral vertical ramus osteotomy8. Some patients may find such proposed permanent solutions to be very aggressive and choose to go for a non-invasive temporary option like botulinum toxin injection. The well-known aesthetic management protocol for a gummy smile is an intramuscular injection of 2.5 U/0.1 ml BTX-A in the Yonsei point9.
There is a huge difference between the social smile and the enjoyment or genuine emotional smile. The first is voluntary, while the latter is involuntary. The differing visual presentations reflect inner emotions, and both are mechanically governed by all the facial muscles of expression10.
The Natura-lip protocol suggests intramuscular injection at the Yonsei point as well as an extra intramuscular injection of 2U/0.1 ml BTX-A in the orbicularis oris muscle to counteract the inward lip inversion.
Materials and methods
This study’s inclusion criteria were excessive gingival display on smiling and loss of the lip bulk when in the relaxed position due to inward inversion of the upper lip secondary to hyper-functional upper lip elevator muscles, as well as skeletal or dental defects causing similar conditions with patients refusing surgery and opting for a non-invasive temporary solution.
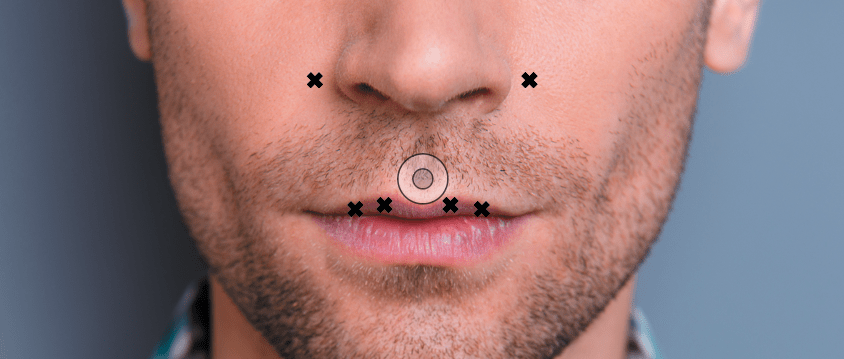
Figure 1 Injections sites across the Yonsei point and orbicularis oris muscle
A group of 20 patients (male and female) between the age of 21–25 were selected to receive the NATURA-LIP injection protocol. During the initial visit, all forms and consents were again explained to each patient, all forms were signed, and the patient’s medical history was reviewed, excluding any subjects with known allergy to botulinum toxin or any condition that contraindicates the use of BTX-A. The trial protocol, risks of the intervention, possible side-effects of BTX-A, and legal rights were presented to the subjects before their participation in the study.
Pre-operative peri-oral close-up photos were taken. Post-operative peri-oral close-up photos were taken two weeks after receiving the treatment protocol in the follow-up sessions. BTX-A was diluted according to the manufacturer’s recommendations to yield 2.5 units per 0.1 mL by adding 4.0 mL normal saline solution to 100 units of vacuum-dried Clostridium botulinum toxin type A.
The injection sites were determined by instructing the patient to mimic the facial expressions responsible for the condition of excessive gingival display (smiling) and palpation on contraction to ensure precise muscle location before injection and detection of any small anatomical variations. No local anaesthesia was administered.
Under sterile conditions, all patients were injected with 2.5U/0.1 ml BTX-A in the Yonsei point and 2U of BTX-A in the orbicularis oris muscle distributed according to Figure 1.
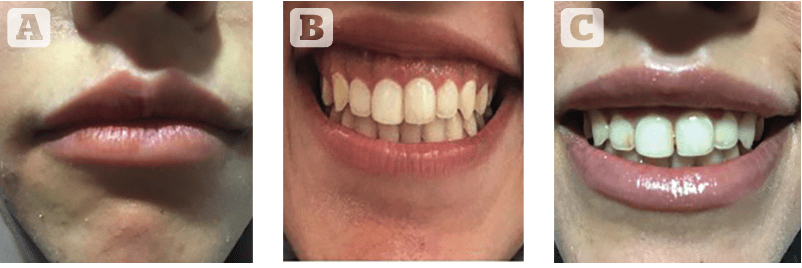
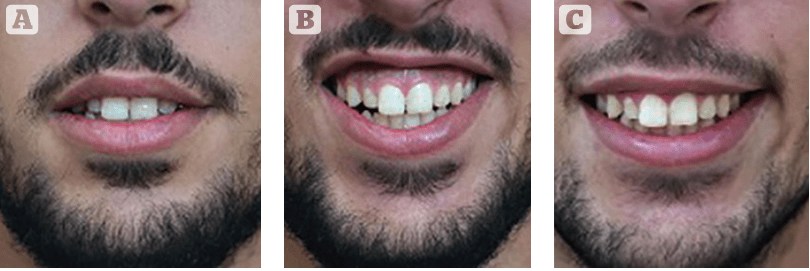
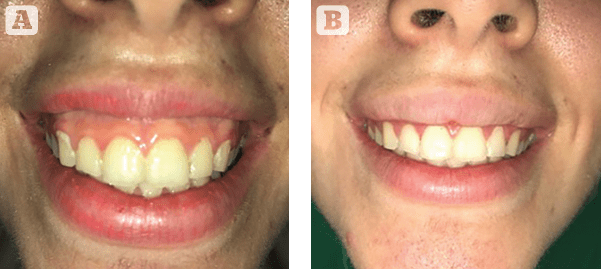
Three of the patients needed further injections of 2U per side of BTX-A in the depressor anguli oris muscle (DAO) to compensate for the sad face or the reverse smile that was previously diagnosed in the first visit. One patient chose to complement the treatment with 3D lip contouring using HA fillers. One patient needed an extra dose of 1U BTX-A injection to camouflage a maxillary canting in the follow-up session 2 weeks post-injection (Figure 2–5).

Results
Twenty patients with hyper-active elevator muscles and inward inversion of the upper lip were enrolled in this study; their age ranged between 21 and 25 years old. Two weeks after botulinum toxin injections of the NATURA-LIP protocol, no complication and no side-effects were noted. Pictures were taken during the follow-up visit 2 weeks post-procedure, and all patients reported an aesthetical improvement to the gingival display and lip bulk preservation during smiling with preserved functions. The patients were recalled every month for follow-up visits.
Discussion
Botulinum toxin has been a great alternative to surgical treatments for neuromuscular disorders since the late 1970s11,12.
Produced by the anaerobic bacterium C botulinum13, it is processed to be a stable, sterile, vacuum-dried powder that, when diluted with a saline solution without preservatives, blocks neuromuscular transmission by binding to acceptor sites on motor or sympathetic nerve terminals, thus inhibiting the release of acetylcholine. When injected intramuscularly at therapeutic doses, BTX-A produces partial chemical denervation of the muscle, resulting in localized reduction in muscle activity13,14.
There are seven serotypes of BTX; the most potent and the most commonly used clinically is type A. Since 1989 the FDA has approved Botox® to be a safe and effective therapy for blepharospasm, strabismus, cervical dystonia, and hemifacial spasm, and, in 2002, it received approval for the treatment of glabellar lines associated with corrugator and procerus muscle activity. Later, in 2004, it obtained approval for the treatment of primary axillary hyperhidrosis. The National Institutes of Health Consensus Conference of 1990 also included it as a safe and effective therapy for other non-labeled uses14.
In this study, we have implemented the knowledge we received from others in the literature to help obtain natural results for patients with an excessive gingival display. Treating the lower part of the face can be as successful as treating the upper part of the face using BTX-A. A thorough knowledge of facial topography and functional anatomy of the facial muscles is key to excellent results and minimizing complications for patients selected to receive BTX-A for aesthetic purposes, especially when dealing with the overlapping peri-oral muscles.
Excellent results were obtained for patients treated with BTX-A for cosmetic indications in the face. Functional evaluation of the facial muscles is essential for an appropriate diagnosis, and knowledge of the topographic and functional anatomy is essential to avoid the most frequent complications of the procedures. The retrospective analysis demonstrated by Sposito15 indicated that when we treat the face as a whole, including the mouth and neck, the doses used in the procedure tend to be higher, and the number of injected sites tends to be greater but injecting the lower face area can be as successful as injecting the upper face area.
Conclusion
The Natura-lip injection protocol to temporarily treat the condition of excessive gingival display allows the patient to restore the lip bulk they have in the relaxed position by adding an extra 2U BTX-A injections in four points along the orbicularis oris muscle. It gives a more aesthetically appealing upper lip when smiling and does not interfere with its function.
Declaration of interest None
Figures 2 & 5 ©Dr Midey Mohammad Helmy;
3–4 © Abdelrahman Shawky
References
- Standring S, Ellis H, Healy JC, Williams A. Gray’s anatomy 40th Edition. Anatomical Basis Of Clinical Practice, Churchill Livingstone, London. 2008;40:415.
- Ackerman MB, Ackerman JL. Smile analysis and design in the digital era. Journal of clinical orthodontics. 2002 Apr;36(4):221-36.
- Peck S, Peck L, Kataja M. The gingival smile line. The Angle Orthodontist. 1992 Jun;62(2):91-100.
- Tjan AH, Miller GD, The JG. Some esthetic factors in a smile. The Journal of prosthetic dentistry. 1984 Jan 1;51(1):24-8.
- Matthews TG, Blatterfein L, Morrow RM, Payne SH. The anatomy of a smile. The Journal of prosthetic dentistry. 1978 Feb 1;39(2):128-34.
- Garber DA, Salama MA. The aesthetic smile: diagnosis and treatment. Periodontology 2000. 1996 Jun;11(1):18-28.
- Fields HW, Proffit WR, Nixon WL, Phillips C, Stanek ED. Facial pattern differences in long-faced children and adults. American journal of orthodontics. 1984 Mar 1;85(3):217-23.
- Shimo T, Nishiyama A, Jinno T, Sasaki A. Severe gummy smile with class II malocclusion treated with LeFort I osteotomy combined with horseshoe osteotomy and intraoral vertical ramus osteotomy. Acta Medica Okayama. 2013;67(1):55-60.
- Polo M. A simplified method for smile enhancement: botulinum toxin injection for gummy smile. Plastic and reconstructive surgery. 2013 Jun 1;131(6):934e-5e.
- Sarver DM, Ackerman MB. Dynamic smile visualization and quantification: Part 2. Smile analysis and treatment strategies. American Journal of Orthodontics and Dentofacial Orthopedics. 2003 Aug 1;124(2):116-27.
- Chaudhary G, Jairath R, Chaudhary N, Chaudhary A, Bector K, Chaudhary G. Rejuvenated Smile with Botox: Opening a new Frontier. Annals of Prosthodontics & Restorative Dentistry. 2016 Apr;2(2):37-41.
- Brin MF, Hallett M, Jankovic J. Scientific and therapeutic aspects of botulinum toxic. Lippincott William & Wilkins; 2002.
- Benedetto AV. The cosmetic uses of botulinum toxin type A. International journal of dermatology. 1999 Sep;38(9):641-55.
- Binder WJ, Blitzer A, Brin MF. Treatment of hyperfunctional lines of the face with botulinum toxin A. Dermatologic surgery. 1998 Nov;24(11):1198-205.
- Spósito MM. New indications for botulinum toxin type A in treating facial wrinkles of the mouth and neck. Aesthetic plastic surgery. 2002 Mar 1;26(2):89-98





{kind=link}