


Dr Agnieszka Surowiecka provides an update on the current use of autologous cell therapy in aesthetic medicine

is a general surgeon with a doctorate in plastic surgery (burns). MedicalSpa Surowiecka
Warsaw, Poland
email: [email protected]
The rising popularity of autologous derived products has been observed not only in sports and regenerative medicine but also in anti-ageing medicine. The main advantage of using biological agents is their natural source. Patients who decide to undergo treatments with the use of autologous methods are eager to achieve a natural, rejuvenating result. A wide range of autologous-derived products allow for a personalised and tailored treatment that meets the expectations of a broad spectrum of patients. Among autologous-derived products, we can distinguish platelet-rich plasma, fibrin, adipose tissue transplants in the form of a micronised fat graft (microfat) or homogenised gel (nanofat), and stromal-vascular fraction (colloquial source of stem cells, SVF). The currently used techniques do not require many hours of laboratory preparations and can be performed immediately in a single procedure.
Autologous conditioned plasma
Autologous conditioned plasma (ACP) or platelet-rich plasma (PRP) is a popular treatment. The main indications for ACP in aesthetics are rejuvenation and fine line correction. It is also frequently used in the combined therapies of alopecia, scars, chronic wounds, hyperpigmentation, and acne. When applied after ablative procedures or surgeries, it accelerates wound healing and convalescence. The most powerful agents in ACP are active platelets. By stimulating fibroblasts, they induce the secretion of collagen, elastin, metalloproteinases (MMP), and self-synthesis of hyaluronic acid. Alpha-granules are responsible for releasing growth factors and cytokines. PDGFs (platelet-derived growth factors) are chemotactic agents for fibroblasts and macrophages, TGF-β (transforming growth factor), EGF (epidermal growth factor), and VEGF (vascular endothelial growth factor) mediate angiogenesis, whereas FGF (fibroblast growth factor) stimulates cell and fibroblast proliferation1-6. D-granules secrete serotonin and ADP.
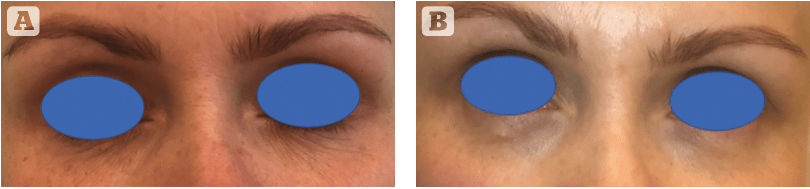
ACP is recommended for application over a number of treatments. In most cases, this consist of three procedures performed every 4 weeks3. After a series of treatments, an improvement in the skin’s condition should be visible. Several studies presented a reduction of wrinkles, improvement in skin tension and elasticity, reduced hyperpigmentation and moderate volumisation that was secondary to skin tightening and reinforcement1–3,7. This effect can also result from the ability to stimulate self-secretion of hyaluronic acid (HA) and increased secretion of collagen type I6. Common indications include the lower eyelid and dermal melanocytosis, which has been known to improve with ACP treatments3,8. After a series of procedures, an improvement in skin density and correction in fine lines is visible (Figure 1). In the case of alopecia, EGF and TGF play the most crucial role by promoting hair follicle maturation. Other agents inhibit cell apoptosis as well4. ACP is successfully used in monotherapy, but when combined with other methods, the spectrum of possibilities escalates. Combined therapies include treatment of post-traumatic scars, where ACP is preceded by ablative lasers or radiofrequency with microneedling6, or acne scars where the use of superficial peelings in one protocol with ACP and microneedling is feasible as well. ACP is a safe and effective treatment. Effects such as redness, swelling, bruising, pain, and burning or itching sensation have been known to occur9, but no severe side‑effects have been reported thus far.
Adipose-derived products
Adipose tissue is often called ‘the Anatomist’s Cinderella’, as it has been neglected for many decades, and its role has been reduced to energy storage, lipogenesis, and lipogenolysis10,11. Meanwhile, it is extremely metabolically and hormonally active. Adipose tissue is the largest endocrine organ, and adipocytes secrete hundreds of growth factors and hormones.
There are also many receptors on the membrane surface of adipocytes regulating their activities, such as receptors for insulin-like growth factors (IGFR-1 and 2), cytokines, thyroid hormones, and vitamin D12. Adipocytes have CXCR4 receptors on their surface, which is known to be a pathway for HIV, but it is also responsible for lipodystrophy in AIDS patients12 and in Crohn’s disease. Adipocytes play an extremely important role in the hair growth cycle. Moreover, 10% of mature subcutaneous tissue adipocytes annually undergo a cycle of transformations, similar to keratinocytes13. Under extreme conditions, such as starvation or shock, a part of the subcutaneous white adipose tissue is transformed into brown adipose tissue (browning effect) and protects the system’s homeostasis and thermoregulation14.
A ACP double syringe has been used (Arthrex Inc. Naples, FL. USA)
Adipose tissue ages. With age, the number of M2 macrophages increases and the number of M1 macrophages decreases, which impairs the neutralization of free fatty acids and leads to the development of atherosclerosis and weight gain. With time, the ability to proliferate and secrete adiponectin also decreases, and the secretion of pro-inflammatory cytokines increases15. This might be the reason why the survival time of fat grafts is still unpredictable, and in elderly patients the final result might be less satisfactory than in younger patients. The final result strongly depends on the patient, and less favourable outcomes of lipofilling in elderly patients might not be connected with poor technique but rather caused by fat tissue ageing.
Physiology
Aside from adipocytes, which constitute 90% of tissue volume, adipose tissue contains numerous other active cells16. The most prominent cells are adipose-derived mesenchymal stem cells (MSCs). They are multipotent cells; however, in vivo, they do not proliferate but act as regulatory cells instead. When allocated to damaged tissue, they stimulate tissue regeneration by secreting growth factors for fibroblasts, endothelium, and anti-inflammatory cytokines. As a result, collagen, elastin, and other proteins of the extracellular matrix are produced. The remodeling of soft tissue is due to metalloproteinases17. Neovascularisation is promoted mainly by pericytes. These are also multipotent cells that do not proliferate in vivo into adipocytes or fibroblasts but coordinate damaged tissue regeneration18. The paracrine dialogue between active cells of fat tissue is commanded by immune cells. They also prevent infection by antigen presentation and humoral or cellular responses. Fat tissue is not only a volumizing agent but also a source of strong and deep tissue regeneration due to the presence of stem cells, pericytes, and adipocytes. That is what makes adipose tissue an excellent alternative to other soft tissue fillers.
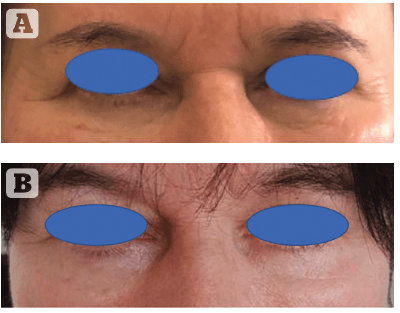
Figure 2 A case of a 60 year-old female. FTA grafting in the lower eyelid, results after 3 moths. (A) Before (B) after.
A ACP double syringe has been used (Arthrex Inc. Naples, FL. USA)
Adipose tissue is characterized by a low risk of rejection and allergies19. Adipose tissue collection is feasible in most cases. Average graft survival rates vary from 10% to 90%20. That is why unpredictable survival rates are considered the main disadvantage of autologous fat transfers. In the early post-transplant period, fat molecules are nourished by osmosis19. Due to the Yoshimura principle, fat particles smaller than 200 µm are the least vulnerable to apoptosis21. When transferring small fat particles, the risk of lumping is also diminished. Most fat-transfer sets available on the market offer devices for fat harvesting and homogenisation that provide the highest quality of fat tissue. Furthermore, adding ACP or stem cells derived from the stromal vascular fraction (CAL-cell assisted lipotransfer) stimulates the process of neovascularisation19,20.
Uses for adipose-derived products
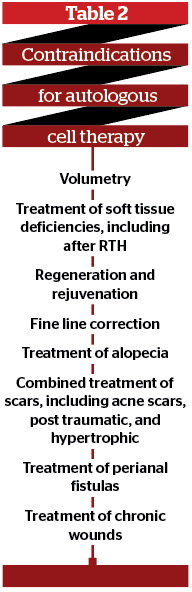
The use of adipose tissue as a soft tissue filler has a long tradition, with the first lipotransfer performed in 1893 by Adolf Neuber. It took a further hundred years for adipose-derived stem cells to be identified22,23. Subcutaneous fat tissue is an ideal source of stem cells. As much as 500 times more stem cells can be harvested from subcutaneous fat compared to bone marrow24. The most common indications for the use of fat transfer and the stromal vascular fraction are presented in Table 1.
Contraindications for autologous cell therapy are listed in Table 2. There are no unequivocal reports or guidelines for autologous cell therapy in oncologic patients. It is known that mesenchymal stem cells do not proliferate in vivo and do not undergo neoplastic transformation25. However, mesenchymal stem cells stimulate angiogenesis; therefore, the risk of stimulating the neoplastic vascular network and promoting metastasis seems to be very high26. One study revealed an improvement in healing and a longer period of remission in head and neck squamous cell carcinoma after the defects in soft tissue had been filled with autologous agents27. On the other hand, there are studies that show the local progression of ductal adenocarcinoma in the breast and accelerated formation of distant metastases28. In aesthetic indications, it is extremely important to take a proper medical history from the patient and examine them thoroughly before the procedure.
An ideal candidate for the transfer of adipose tissue would be a patient who requires a large volume of restoration as well as strong rejuvenation and regeneration of the skin, with subcutaneous adipose tissue at the donor site feasible for harvesting. The second-best group may be patients with failed hyaluronic acid fillers in the area of the lower eyelid and a tear through. In experienced hands, fat grafting involves a lower risk of lumping and overcorrection than hyaluronic acid29. Strong regeneration and tightening of the skin, as well as improvement of dermal melanocytosis in the lower eyelid area, can be amplified, and satisfactory long-term results can be achieved by adding mesenchymal stem cells to the fat graft9,30–32. Figure 2 presents a case of a strong rejuvenation in the lower eyelid after the transfer of 1.5 ml of homogenized fat graft (nanofat), covered with 1 ml of stromal-vascular fraction per site. Improvement in volume, as well as correction of fine lines, enhanced skin tone, and elasticity are visible.
Safety profile
The effects of using adipose tissue, despite the large volume, are very natural. However, it should be remembered that these are more invasive procedures, with the risk of complications and imposing a long learning curve on the operator. According to FDA restrictions, autologous products permitted for use in aesthetics must not be manipulated, cannot be combined with external agents, as well as need to be homogenous and used in the same procedure. The most common side effect is swelling, which may persist for up to a month after the procedure. The literature describes cases of graft migration, the formation of calcifications and cysts, as well as ischemia, necrosis, and vision loss. Extreme care should be taken when administering adipose tissue, with a careful assessment of the patient’s anatomy and the use of cannulas. It is recommended to administer slightly overcorrect deposits, as a part of the graft will be absorbed. Complications may also be related to the tissue extraction process. One should not forget about the risk of fatty embolism and thrombotic complications as well33.
The methods for safe and effective fat transfer are still at the development stage. Some future trends have been recently discussed. One of the most promising innovations in biological treatment might be cryopreservation. Fat removed during an elective liposuction can be frozen, stored, and used on-demand within several years. Allogenic fat transfers also seem to be an interesting alternative; however, the immunogenicity of fat tissue could prove a serious burden. Efforts are being made to develop various scaffolds and growth factors that could be safely added to fat grafts to improve their survival34. Finally, there are observations that simple techniques, like botulin, can have a beneficial influence on fat grafting results. By relaxing the moving parts of the face before transferring fat, the mechanical stress of the muscles is diminished, and fat particles are believed to last longer35.
Conclusions
The growing interest among doctors and patients in autologous cell therapy in anti-ageing medicine has resulted in an increasing number of reports and demand for treatments. It is a direction that is dynamically developing and improvements appear every year. Biological agents are a strong alternative to fillers and biostimulators. The means of their action in the skin are far beyond the possibilities of synthetic products and extremely fascinating as well.
Declaration of interest None
Figures 1–2 © Dr Surowiecka
Tables 1-2 © Dr Surowiecka
References
- Graziani F, Ivanovski S, Cei S, Ducci F, Tonetti M, Gabriele M. The in vitro effect of different PRP concentrations on osteoblasts and fibroblasts. Clin Oral Implants Res 2006;17:212-219
- Anitua E, Sánchez M, Zalduendo MM, de la Fuente M, Prado R, Orive G, Andía I. Fibroblastic response to treatment with different preparations rich in growth factors. Cell Prolif 2009;42:162-170
- Maisel-Campbell, A. L., Ismail, A., Reynolds, K. A., Poon, E., Serrano, L., Grushchak, S., Farid, C., West, D. P., & Alam, M. (2020). A systematic review of the safety and effectiveness of platelet-rich plasma (PRP) for skin aging. Archives of Dermatological Research, 312(5), 301-315. https://doi.org/10.1007/s00403-019-01999-6
- Alves R, Grimalt R: A Review of Platelet-Rich Plasma: History, Biology, Mechanism of Action, and Classification. Skin Appendage Disord 2018;4:18-24. doi: 10.1159/000477353
- Stevens, H.P. ACA-Technik: „stromal vascular fraction“, „platelet-rich plasma“ und Mikrofett zur körpereigenen Regeneration und Hautverjüngung. J Ästhet Chir 12, 77–83 (2019). https://doi.org/10.1007/s12631-018-0151-6
- Elghblawi, E. Platelet‐rich plasma, the ultimate secret for youthful skin elixir and hair growth triggering. J Cosmet Dermatol. 2018; 17: 423– 430. https://doi.org/10.1111/jocd.12404
- Motosko CC, Khouri KS, Poudrier G, Sinno S, Hazen A. Evaluating Platelet-Rich Therapy for Facial Aesthetics and Alopecia: A Critical Review of the Literature. Plast Reconstr Surg 2018;141(5):1115-1123.
- Aust M, Pototschnig H, Jamchi S, Busch KH. Platelet-rich Plasma for Skin Rejuvenation and Treatment of Actinic Elastosis in the Lower Eyelid Area. Cureus 2018;10(7):e2999
- Surowiecka A, Pototschnig H, Can hydrogel dressings reduce patiens’ discomfort and side effects of facial platelet-rich plasma injections?, Deramtological Therapy, June 2020, https://doi.org/10.1111/dth.13906
- Trayhurn, P. (2005), Endocrine and signalling role of adipose tissue: new perspectives on fat. Acta Physiologica Scandinavica, 184: 285-293. doi:10.1111/j.1365-201X.2005.01468.x
- Pond CM. Adipose tissue, the anatomists’ Cinderella, goes to the ball at last, and meets some influential partners. Postgrad Med J. 2000;76(901):671–673. doi:10.1136/pmj.76.901.671
- Peyrin-Biroulet L, Chamaillard M, Gonzalez F, et al. Mesenteric fat in Crohn’s disease: a pathogenetic hallmark or an innocent bystander?. Gut. 2007;56(4):577-583. doi:10.1136/gut.2005.082925
- Kruglikov IL, Zhang Z, Scherer PE. The Role of Immature and Mature Adipocytes in Hair Cycling. Trends Endocrinol Metab. 2019;30(2):93-105. doi:10.1016/j.tem.2018.11.004
- M. Chondronikola, L.S.Sidossis, Brown and beige fat: From molecules to physiology, Biochimica et Biophysica Acta (BBA) – Molecular and Cell Biology of Lipids, 2019, Vol: 1864, Issue: 1, Page: 91-103
- Y.Panx, R. Yuan, X. Yang, Z. Qi, Adipose tissue, aging, and metabolism,Current Opinion in Endocrine and Metabolic Research, 2019, Vol: 5, Page: 11-20
- Shukla et al. Adipose-derived stem cells in radiotheraphy injury: a new frontier, Frontiers in Surgery, 2015:2(1);1-12
- Gimble JM, Katz AJ, Bunnell BA. Adipose-derived stem cells for regenerative medicine. Circ Res. 2007;100(9):1249-1260. doi:10.1161/01.RES.0000265074.83288.09
- Esteves CL, Donadeu FX. Pericytes and their potential in regenerative medicine across species. Cytometry A. 2018;93(1):50-59. doi:10.1002/cyto.a.23243
- Wei H, Gu SX, Liang YD, et al. Nanofat-derived stem cells with platelet-rich fibrin improve facial contour remodeling and skin rejuvenation after autologous structural fat transplantation. Oncotarget. 2017;8(40):68542-68556. Published 2017 Jul 31. doi:10.18632/oncotarget.19721
- Modarressi A., Platlet Rich Plasma (PRP) Improves Fat Grafting Outcomes. World J Plast Surg. 2013;2(1):6-13
- Eto H, Kato H, Suga H, et al. The fate of adipocytes after nonvascularized fat grafting: evidence of early death and replacement of adipocytes. Plast Reconstr Surg. 2012;129(5):1081-1092. doi:10.1097/PRS.0b013e31824a2b19
- Suh A, Pham A, Cress M, et al. Adipose-derived cellular and cell-derived regenerative therapies in dermatology and aesthetic rejuvenation, Aging Research Reviews, 54 (2019), 1000933
- van Dongen J, Gostelie O, Vonk L, et al. Fractionation of Adipose Tissue Procedure With a Disposable One-Hole FractionatorAesthetic Surgery Journal, Volume 40, Issue 4, April 2020, Pages NP194–NP201
- Bacakova L, Zarubova J, Travnickova M, et al. Stem cells: their source, potency and use in regenerative therapies with focus on adipose-derived stem cells – a review, Biotechnology Advances, 2018 Jul-Aug 2018;36(4):1111-1126.
- Strużyna J, Pojda Z, Zastosowania komórek macierzystych z tkanki tłuszczowej w medycynie regeneracyjnej, Chirurgia Plastyczna i Oparzenia, 2015;3(4):151–157
- Rubio D, Garcia-Castro J, Martín MC et al. Spontaneous human adult stem cell transformation. Cancer Res 2005;65(8):3035–3039.
- Danan D, Lehman C, Mendez R et al. Effect of Adipose-Derived Stem Cells on Head and Neck Squamous Cell Carcinoma
- Goto H, Shimono Y, Funakoshi Y, et al. Adipose- derived stem cells enhance human breast cancer growth and cancer stem cel-like properies throught adipsin, Oncogene 2018
- Bernardini F, Gennai A, Izzo L, et al. Superficial Enhanced Fluid Fat Injection (SEFFI) to Correct Volume Defects and Skin Aging of the Face and Periocular Region,Aesthetic Surgery Journal 2015, Vol 35(5) 504–515
- Tonnard P, Verpaele A, Peeters G, et al. Nanofat grafting: basic research and clinical applications. Plast Reconstr Surg. 2013; 132: 1017-1026.
- Azzam A, Kholosy H, Abouarab M; The efficacy of autologous Nanofat Injections in the treatment of infraorbital dark colouration; Egyp.J.Plast.Reconstr.Surg., Vol 43, No. 3, October 445-452, 2019
- Jiang S, Quan Y, Wang J, Cai J, Lu F. Fat Grafting for Facial Rejuvenation Using Stromal Vascular Fraction Gel Injection. Clin Plast Surg. 2020;47(1):73-79. doi:10.1016/j.cps.2019.09.001
- Wang JV, Schoenberg E, Saedi N, Ibrahim O. Platelet-rich Plasma, Collagen Peptides, and Stem Cells for Cutaneous Rejuvenation. J Clin Aesthet Dermatol. 2020;13(1):44-49.
- Xiong S, Yi C, Pu L, An Overview of Principles and New Techniques for Facial Fat Grafting, Clin Plastic Surg 47 (2020) 7–17
- Wolf DA, Beeson W, Rachel JD, et al. Mesothelial Stem Cells and Stromal Vascular Fraction for Skin Rejuvenation. Facial Plast Surg Clin North Am. 2018;26(4):513-532. doi:10.1016/j.fsc.2018.06.011



{kind=link}