


Dr Elena Fasola discusses a new treatment for stretch marks
Commonly called Stretch marks, striae distensae (SD) are linear, erythematous or atrophic form of dermal scarring. They manifest themselves by favouring certain areas of the body which, due to genetic factors added to para-physiological or pathological factors, are subjected to an increase in the volume of subcutaneous tissues caused by weight gain or muscle growth or by the increase in volume of some internal organs, such as during pregnancy. This increase in volume stresses the overlying skin to the point where the collagen fibres break.
As soon as they are formed, in their florid phase, they are characterised by an erythematous to violaceous colour, they are often in relief on the skin surface, but over time they tend to evolve towards an hypopigmented lesion, of pearly-with colour, with scarring meaning; they are respectively called: striae rubra and striae alba. The most affected regions are the thighs, the hips, buttocks, abdomen, medium upper arm, lower back and breasts. They can occur in both sexes and at any age, but are very common in women between the ages of 15 and 30, particularly during puberty and pregnancy1.
Although asymptomatic, striae distensae may be psychologically distressing to patients. Various topical and procedural modalities have been employed for the treatment of striae distensae and until now, their treatment was mainly a preventive type thanks to the maintenance of a normal weight possibly for life, thus avoiding sudden changes in volume; medical-aesthetic treatments, on the other hand, are almost always of the combined type, using two or more of these methods together. Laser and other light-based devices and topical treatments are the most commonly applied interventions. These are equally effective and there is no significant difference between them in side-effects and treatment duration. Combination therapy of two or more modalities is usually better than using each one alone.
Striae distensae epidemiology and risk factors
Epidemiologic data on SD in the general population are limited. Reported incidences have ranged from as low as 11% in normal men to up to 88% in pregnant females3. Predisposing factors include pregnancy, adolescent age4, drug exposure (e.g., topical or systemic corticosteroids), underlying disease (e.g., Cushing’s syndrome), and surgery (e.g., breast augmentation)5.
Aim of the study
We are evaluating the efficacy of a single method of treating atrophic striae distensae (striae alba), through multiple injections of low molecular weight HA added to a specific mixture of AA (Glycine, L-Proline, L-Lysine, L-Leucine, L-Alanine, L-Valine–HY6AA, SuneKos® Body, Professional Dietetics), in various anatomical areas of the body affected by SD Alba. The production of collagen and elastin allows us to give greater elasticity to the dermis and probably presuppose the prevention of the formation of new stretch marks.
Inclusion criteria provided 20 healthy adult volunteers with BMI <32 Kg/m2, with hypotrophic striae distensae (striae albe) affecting derma of one or more of the following anatomical areas: breast, arms, abdomen, inner thigh, inner knee, trochanteric area, gluteal area, posterior supra-iliac area and lumbar area. Patients with auto-immune soft tissue diseases, with ongoing anti-inflammatory therapy, inflammatory or infection diseases affecting treatment area or with presumed or confirmed sensitivity towards one of the contents or ingredients of the product were excluded from the study.

Materials and methods
The open clinical trial is conducted by one centre under dermatological control.
The study is conducted on 20 healthy adult volunteers, age range 18–60 years, whose informed consent has been obtained. 10 ml Sunekos Body, is injected four times at intervals of 2 weeks each.
Efficacy evaluations are performed at (T0), at T4 (after 8 weeks) and at T5 12 weeks after treatment with I-Phone-Photo and use of GAIS (Global Aesthetic Improvement Scale) and PSDQ (Physical Self-Description Questionnaire) scales.
Technique
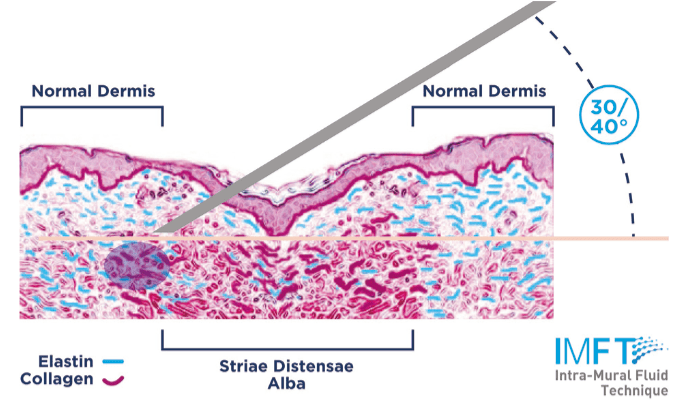
The injections are performed by 30–32G needle, with a Intramural Fluid Technique (ImFT), directly into the wall of every single ASD, with needle inclination angle of 30–40 degrees, every point of injections will be performed at a distance of 3–4 mm, the volume of injected product is 0.2–0.4 ml.
Preliminary results
Results are encouraging: after the second injection with GAIS scores after treatment of 3. In addition to visibly reducing the striae albe, the tone of the surrounding skin greatly improves preventing the formation of new stretch marks.
References
- Jennifer L MacGregor, MDNaissan, O Wesley, MD – Striae distensae (stretch marks) – Uptodate 2021
- Seirafianpour 1, S Sodagar 1, S Mozafarpoor 2, H R Baradaran 3 4, P Panahi 1, B Hassanlouei 5, A Goodarzi. Systematic review of single and combined treatments for different types of striae: a comparison of striae treatments J Eur Acad Dermatol Venereol. 2021 May 22.doi: 10.1111/jdv.17374.Online ahead of print. 6PMID: 34021922
- Ghasemi A, Gorouhi F, Rashighi-Firoozabadi M, et al. Striae gravidarum: associated factors. J Eur Acad Dermatol Venereol 2007; 21:743.
- Sybert VP. Striae in adolescent males. Pediatr Dermatol 2010; 27:576.
- Basile FV, Basile AV, Basile AR. Striae distensae after breast augmentation. Aesthetic Plast Surg 2012; 36:894.



