



Dalvi Humzah, Antonello Tateo, and Gabriel Siquier discuss using a stable hybrid cooperative complex hyaluronic acid to treat the neck
THE APPEARANCE OF THE NECK IS currently one of the main points of interest of the aesthetic field; there are many changes to this area with ageing that require addressing with a multi-modal approach. In youth, the neck is clearly defined with smooth non-creased skin, visible structures of the medial and lateral borders of the sternocleidomastoid, and posteriorly the borders of trapezius with hollows at the suprasternal notch and supraclavicular areas1. During the process of ageing there are visible changes in the skin texture, underlying platysmal muscle changes, and volumetric changes in the fat layers.
This initially results in visible crease lines and progressive muscle hypertonicity, which leads to attenuation of the mandibular definition and platysmal bands. There is further progressive deterioration of the skin texture and quality with associated loss of dermal structures. The associated loss of collagen and elastin causes further sagging and skin laxity2. There have been studies made to quantify the amount of fat in the neck;3,4,5 it appears that the volumetric changes associated with the neck is an interplay of the subplatysmal and pre-platysmal fat pads. Other authors have described three compartments of subplatysmal fat: central, medial, and lateral2. How these various fat pads within the neck change with ageing is not described. When analysing the neck in the aesthetic patient, there are three specific parameters to consider:
- The degree of skin laxity/sagging (with/without the formation of ‘creases’): appear as fine lines that run parallel to each other as ageing progresses
- Necklace lines: horizontal crease lines etched into the skin. They tend to deepen and look more noticeable with age and appear as the first sign of ageing
- Platysmal bands: the platysma contracts with age which causes blunting of the sharp jawline and vertical neck bands in the area.
- Using these parameters the neck may be classified into three separate groups:
- Group 1: textural changes (increased laxity) of the skin with or without necklace lines
- Group 2: as Group 1, with platysmal bands and or loss of jawline contour
- Group 3: as Group 2 with necklace lines, platysma hypertonicity, and advanced skin laxity/sagging.
In treating these different groups, we propose a multi-modal approach using 32 mg/ mL of stable hybrid cooperative complexes of high and low molecular weight hyaluronic acid (Profhilo®, IBSA Farmaceutici Italia, Srl) alone and in combination with botulinum toxin type A.
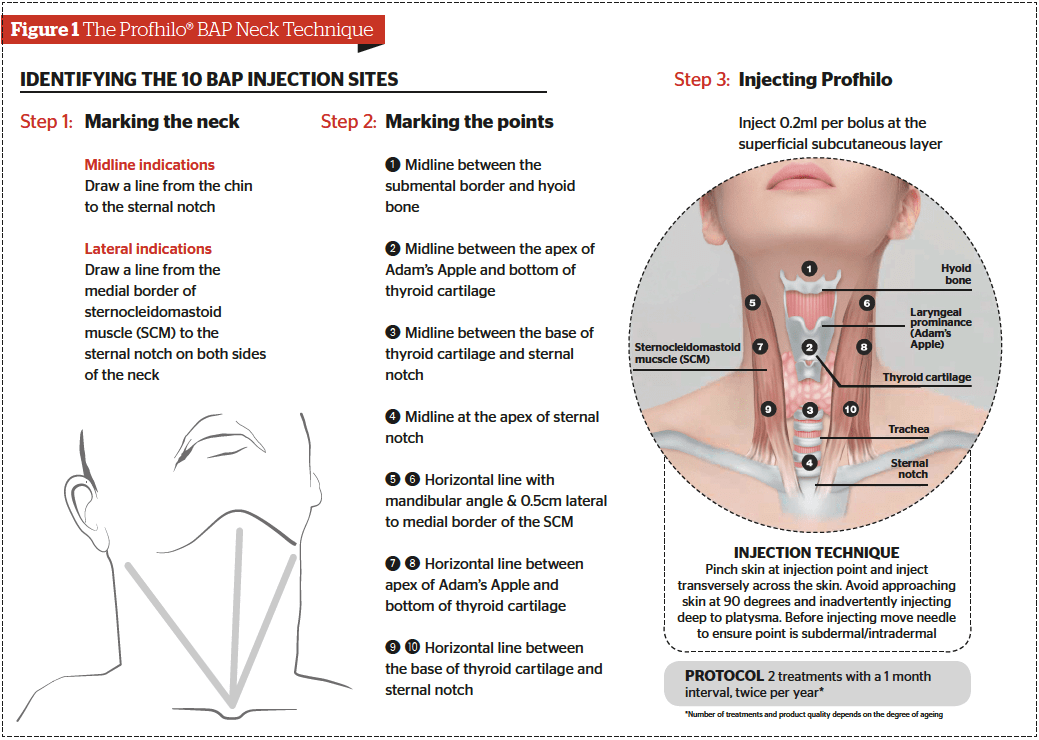
Group 1: Profhilo® BAP neck technique
The neck was injected according to the BAP Neck Technique with 2.0 mL of Profhilo® with a month between the two treatments. The 10 point BAP Neck Technique was developed in order to provide reproducible points of injection and to standardise these points irrespective of variations between patients and ensure that the injection points avoid potential injury to vital structures (Figure 1).
Group 2: Botulinum toxin and Profhilo®
At the first session, a total of 50 IU of botulinum toxin was injected into the platysmal bands and horizontal lines (if present) using the following protocol: on the platysmal bands, 2 U per point was injected every 1–2 cm in a relaxed state with a subdermal bolus technique. On the horizontal wrinkles, 1–2 U per point was injected every 1–2 cm using an intradermal bolus technique in the mandibular platysma (Nefertiti Lift)6. Then two 2.0 mL doses of Profhilo® were injected at day 15 and day 45, respectively. Profhilo® was injected according to the BAP Neck Technique (10-point injections of 0.2 mL) (Figure 1).
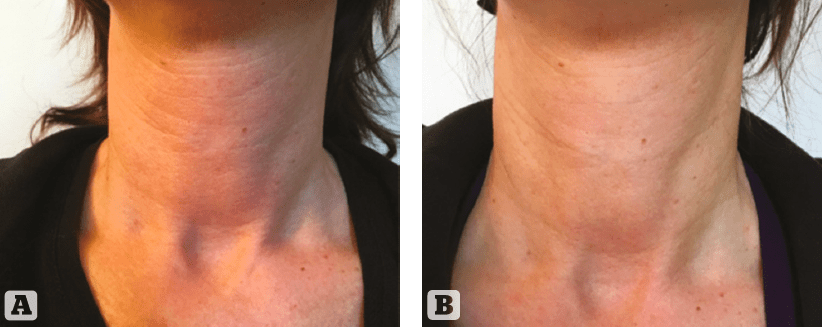
Figure 3 (A) Group 1 Before and (B) After treatment
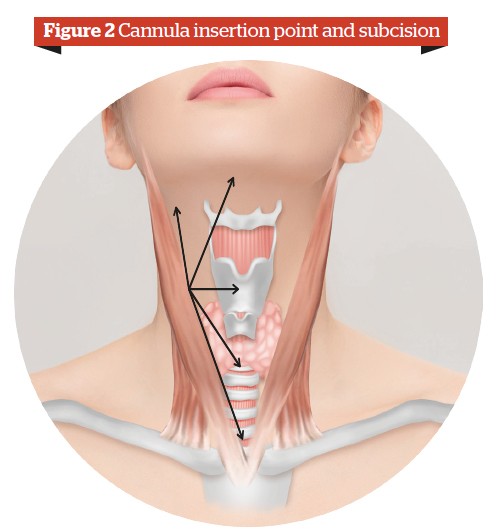
Group 3: Botulinum toxin and Profhilo® — cannula subcision
This group had a similar treatment with botulinum toxin A. On day 15 and day 45 Profhilo® was administered with a 25 G 50 mm (TSK Steriglide) cannula: an insertion point was made 1 cm lateral to the anterior border of the sternocleidomastoid muscle, a total of 5 passes in the pre-platysmal plane (0.2 mL per thread) from the following points towards the insertion point in a retrograde line (Figure 2):
- Angle of jaw
- Mentum
- Thyroid cartilage
- Tracheal cartilage
- Sternal notch.
Personal experience We tested these three techniques with a total of 20 patients per group. All patients in these groups experienced a continuous, gradual effect with a significant clinical improvement in neck ageing. The treatment was well tolerated and the patients were very satisfied with the overall aesthetic outcome and the duration of the results. Figures 3–5 demonstrates before and after examples from each group.

Figure 4 (A) Group 2 Before and (B) After treatment
Discussion
Profhilo® is a novel HA preparation based on stable, cooperative, hybrid complexes, which is the first product developed by NAHYCO® Hybrid Technology, an innovative thermal production process patented by IBSA. The production involves a mixture of 32 mg of high molecular weight HA (1100–1400 kDa) and 32 mg of low molecular weight HA (80–100 kDa). This mixture is then stabilised by a thermal process, which does not use cross-linking agents. The characteristics of Profhilo® are:
- High HA concentration (64 mg/2 mL)
- High manageability
- Optimal tissue diffusion
- Low viscosity
- No BDDE or other chemical agents
- Low inflammatory response
- Thermally stabilised natural HA with a duration similar to a weakly cross-linked gel.
Profhilo® infiltration results in a multilevel dynamic remodelling and is indicated for tissue bio-remodeling7. The effectiveness of Profhilo® in improving the extracellular environment was shown to:
- Maintain optimal conditions for fibroblast, keratinocyte, and adipocyte vitality
- Favour a remodelling of the extracellular matrix in terms of elasticity and support7.
Botulinum toxin type A is a frequently used tool within the therapeutic spectrum for the treatment of hyperkinetic facial wrinkles, including those in the areas of the mouth and neck8. With ageing, the platysma muscle becomes hyperkinetic and hypotonic which results in vertical muscle bands and horizontal neck lines. The platysma muscle stretches the skin of the neck downward and, with the action of the depressor anguli oris, pulls down the lateral corners of the mouth.
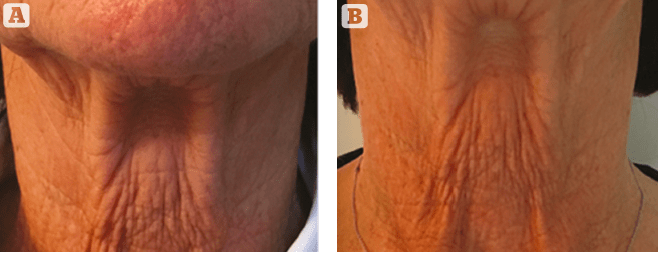
Figure 5 (A) Group 3 Before and (B) After treatment
Botulinum toxin can be used on its own or in conjunction with other procedures. It is particularly useful in patients with platysma muscle hyperactivity6. Therefore, the combination treatment with Profhilo® and botulinum toxin type A can be considered a good multi-modal approach to improve the overall quality of the neck.
Conclusion
In aesthetics there is an increasing interest in treating the ageing neck; the youthful neck includes clear skin texture and tone without laxity. The ageing process involves loss of volume, increased skin laxity, worsening texture, and wrinkling. The aesthetic treatment of the neck is of crucial importance in the overall rejuvenation programme.
This multi-modal approach improved the aged skin of the neck, reducing skin laxity and increasing elasticity and consistency of superficial soft tissues. Based on this preliminary experience, botulinum toxin type A and stable hybrid hyaluronic acid cooperative complexes when used in combination are effective and safe.
Declaration of interest The authors declare that IBSA Farmaceutici Italia Srl provided support to the preparation of the manuscript
Figures 1-2 © IBSA; 3-5 © Dr. Siquier
References:
- Ellenbogen R, Karlin JV. Visual criteria for success in restoring the youthful neck. Plast Reconstr Surg. 1980;66:826-837
- Bazin R, Doublet E. Skin Aging Atlas: Volume 1. Caucasian Type. Paris, France: Med’Com Editions; 2007
- Adamson J, et al. The surgical correction of the “turkey gobbler” deformity. Plast Reconstr Surg. 1964;34:598-605
- Raveendran SS, et al. An Anatomic Basis for Volumetric Evaluation of the Neck. Aesthetic Surgery Journal 2012;32(6): 685 –69
- Renaut A, et al. Distribution of submental fat in relationship to the platysma muscle. Oral Surg Oral Med Oral Pathol. 1994;77:442-445
- Jabbour SF, et al. Botulinum Toxin for Neck Rejuvenation: Assessing Efficacy and Redefining Patient Selection. Plast Reconstr Surg. 2017;140:9e-17e
- Agolli E, et al. Hybrid cooperative complexes of high and low molecular weight hyaluronans (Profhilo®): review of the literature and presentation of the VisionHA project. Dermatological Experiences 2018 DOI: 10.23736/ S1128-9155.18.00470-3
- Spósito MM. New indications for botulinum toxin type a in cosmetics: mouth and neck. Plast Reconstr Surg. 2002 Aug;110(2):601-11; discussion 612-3




{kind=link}