


Use of minimally-traumatic harvesting and handling techniques
Fat transplant survival depends on the instrumentation used for harvesting and placement of the fat graft. Damage to the fat graft is inversely related to the diameter of the instruments used to extract and inject. A large diameter cannula for harvesting and small diameter for placement can destroy the fat graft; therefore, it is paramount to use the same diameter for both procedures.
The pressure generated when injecting fat increases as a function of decreasing needle diameter, hence more pressure and more destruction of the grafted tissue.When using cannulae less than 2 mm in diameter, there is a decrease in the metabolic activity of the fragments and alteration in the anatomy of the graft. With the use of low-vacuum pressure, the closed syringe technique for harvest, using the correct cannula for harvest (cobra) and transfer (blunt, one hole), fat grafting (large and small volumes) has become more effective and better understood. (The closed syringe technique consists of using various sized luer lock syringes in combination with adequate cannulae in fat harvesting to avoid any exposure to air. After more than 20 years’ experience in performing lipografting, the author feels the closed syringe technique is adequate, easy and safe to use. Of course, this implies adequate knowledge, training and experience of the surgeons using the technique.)
When discussing fat transplant survival, the presence of blood in the injected fat stimulates macrophage activity, which can decrease the number of fat cells. It is mandatory then, to thoroughly clean the harvested fat in order to remove all of the blood: never use fat containing blood for grafting. The Coleman technique can be used, with centrifugation at 3000 rpm for 3 minutes; or decantation (washing the cells in a physiological solution) prior to injection until the infranatant solution is transparent. It is also possible to use the newer devices for harvesting fat tissue, which claim to clean the fat tissue for immediate use. These systems, however, overlook the importance of the presence of lidocaine in the tumescent anaesthetic solution. It is well known that solutions containing lidocaine are very lipophilic13–17.
However, the presence of high concentrations of intracellular anaesthetic solutions in grafted adipocytes is among the potential negative factors in the global success of the graft. Therefore, the reasonable reduction of intracellular lidocaine levels is considered advantageous. Lidocaine still exists within the adipocyte, even after three separate rinses using a normal saline solution. In smaller and larger volume transfers, such as breast and buttock areas, rinsing and the addition of PRP is now favoured.
Proper preparation of the recipient bed
Max Lafontan, one of the world leaders in the physiology of fat tissue, answered questions about fat grafting11,18,19:
- Is it true that grafted fat survives the first 2 days through osmosis and then develops microcirculation? Fat grafts survive for a while in the new environment through exchanges with the extracellular fluid. (NB. Initially the fat graft is highly hypoxic. During this period, secretion of a number of proangiogenic factors is initiated in the adipocytes, preadipocytes and endothelial cells. It is this process that facilitates the development of the microcirculation.)
- Is it important that grafted fat is in contact with normal fat tissue in the grafting area (recipient zone)? Optimised contact of the graft with the surrounding tissue is essential for rapid build-up of new vessels, which feed adipocytes and preadipocytes. Larger pieces of fat rapidly become necrotic in the centre of the graft owing to increased hypoxia. (This emphasises the importance of using a number of smaller grafts in different levels of the normal fat tissue.)
One technique that can increase the pO2 in the tissue surrounding the graft is the use of carboxytherapy at the area for grafting 3 weeks prior20–25. The effects of carboxytherapy are:
- Increased tissue oxygenation (increase the pO2)
- Increased flow rate and vasodilatation (in the vessels)
- Increased collagen in the connective tissue.
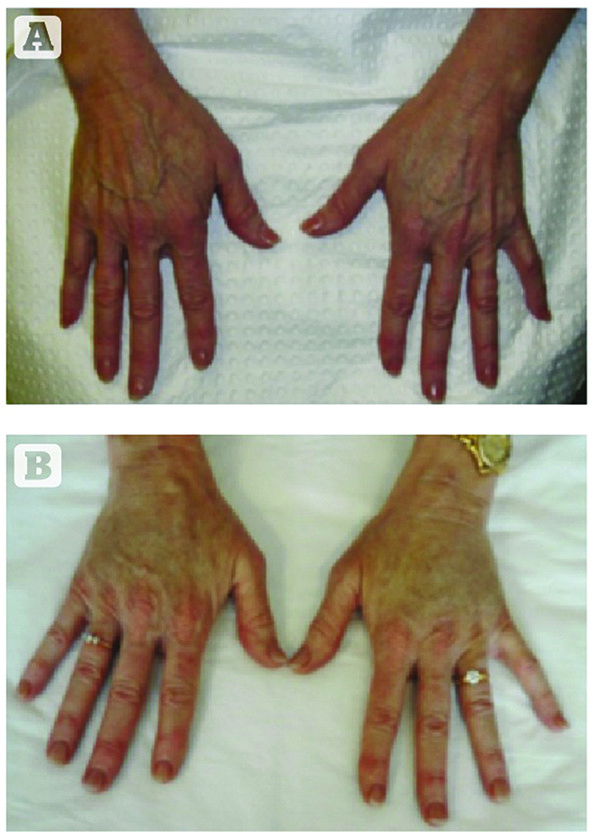
Figure 3 Hand rejuvenation with lipografting, (A) before and (B) after
The use of carboxytherapy is based on subcutaneous injection of CO2. Following the explanation of Max Lafontan regarding the importance of the concentration of oxygen in the recipient area and the hypoxic state of the donor fat tissue, the author uses carboxytherapy to enhance the concentration of oxygen in the recipient area11,18,19.
The recipient site provides the needed circulation and cellular access for structural cells, healing cells, and integral capillaries. It has been suggested that this may explain why small aliquots of graft placed in prepared tunnels, and surrounded by native fat and stromal cells, contribute to and enhance graft survival and success.
In the presence of normal oxygen tensions, the number of fibroblasts and amount of collagen deposits — as well as the number of capillaries — can be increased by increasing the number of macrophages present (i.e. through the liberation of growth factors from the macrophages). More than 20 years of experience confirms that small and large volume (breast, buttocks, extremities) augmentation using autologous fat grafting can be safely, predictably, and effectively accomplished.
Survival
The survival of free fat used as autograft is operator‑dependent. It requires delicate handling of the graft tissue, careful washing of the fat to minimise extraneous blood cells, and installation into a site with adequate vascularity. One of the most important influences of grafting adult lipocytes (plus stimulation of rich mesenchymal stem cell components within the fat tissue) is the addition of platelet-derived factors added to the harvested graft materials prior to graft placement.
Complications of fat augmentation
Controversy with regard to the efficacy of autologous fat grafting seems related to the amount of graft retained and the long-term retention of volume increase. Many claim relatively high reabsorption rates (30–60%), which do not account for the fluid volume used to transport graft cells from donor to recipient sites. During the first week there is reabsorption of the liquid, including that used for tumescent anaesthesia. Other complications may include27–32:
Minor complications
- Need for repeat injection
- Bruising
- Haematoma
- Swelling
- Prolonged erythema
- Tenderness and/or pain
- Fibrous capsule
- Infection (rare)
- Mass (e.g. fat cyst from too much fat in one place)
- Microcalcifications.
Major complications
- Loss of sight from retinal artery occlusion, owing to injection at the glabella area
- Central nervous system damage, particularly at the glabella area
- Pulmonary embolism.
However, the loss of fat volume is the most common problem in fat transfer. Prior to fat transplantation, the patient should be informed of this possibility and the need for reinjection. Unilateral blindness has been reported in four cases, with severe central nervous system damage in one case following fat injection to the glabella area.
Retrograde embolisation can occur in the frontal and dorsal nasal arteries, which are supplied by the ophthalmic artery, a branch of the internal carotid artery33. The ophthalmic artery supplies the ocular group, comprising the central retinal artery, short posterior ciliary artery, long posterior ciliary artery, and the anterior ciliary artery. The cerebral portion of the internal carotid artery supplies the anterior cerebral artery, middle cerebral artery, posterior communication artery, and the choroidal artery. Fat tissue entering the frontal and dorsal nasal arteries may gain retrograde access to the eye and brain. Feinendegen DL et al concluded that the applied force and velocity of injections are important factors for ocular and cerebral fat embolism34.
There are many recognised factors with substantial influence on the success of autologous fat transplantation, some of which include35:
- The patient’s systemic health
- Genetic predisposition for cellular fat storage from the preferred donor sites (so-called ‘primary’ fat deposit locations)
- Pre- and post-grafting patient nutrition
- Basal metabolic rate
- Use of minimally-traumatic harvest and handling techniques
- Correct preparation of the recipient bed
- Relative early graft immobilisation at the recipient sites during the initial graft acceptance and initiation of the healing cascade.

