


Managing expectations
Aside from the obvious limitations of genetics, skin, anatomy, and health factors, there are also patient expectations that make 100% success a near impossibility. Practitioners who make absolute promises or guarantees like ‘I can make your nose perfectly straight’, or ‘I’ll take away all your wrinkles’, are walking a fine line. To promise anything near perfection or an outcome that cannot always be delivered, is
wholly misleading.
In order for patients to appreciate a good result, it is important to educate them about what good versus poor cosmetic results are. Most patients really don’t know what constitutes ‘bad’ BOTOX® or over-filled lips. Among the reasons that most patients don’t zero in on good results is that when treatments are well executed they are often undetectable, so they simply cannot identify that someone has had anything done.
The era when it was perfectly acceptable to simply tell patients what to expect from a cosmetic treatment is long since gone, as is simply showing them in a mirror. Having a robust selection of before and after photographs of actual patients are an absolute necessity now. Patients demand to see photos today, and preferably not just the photos provided by filler and laser companies. It is imperative to show patients that results can be achieved from each treatment offered in the clinic.
Deflecting angry patients
One of the key roles of an effective staff is to identify the early signs of a problem patient and alert the doctor while there is still time to intervene. The relationship between a practitioner or a clinic and a patient can go pear-shaped very quickly if you are not paying attention. Regrettably, the Internet is full of patients who post that another doctor was ‘horrified by what they looked like’, and ‘couldn’t believe anyone would do that’. These tales are frequently exaggerated; however, sometimes there is a kernel of truth buried under the hyperbole. Doctors who are inclined to criticise other doctors’ work indiscriminately are perpetuating this phenomenon.
Unexpected post-treatment events often require rapid intervention, no matter how seemingly insignificant they may appear to the trained eye. It is important to preserve the distinction in your own mind between a ‘problem patient’ and ‘a patient with a problem’. While both present the risk of potential litigation and should be handled with kid gloves, the latter deserves your utmost care and attention rather than your unspoken wrath.
A patient who comes in for his/her first follow-up visit with a sad, sullen look may just be anxious about the healing process, but this could also be a precursor of things to come. A soothing touch, kind demeanor, and a genuine display of interest in his/her problem may distill any ill will. The best opportunity you will ever have to turn an unhappy patient around is at the moment you suspect that the patient has become disenchanted with your services. Failure to act is tantamount to facilitating a bad outcome. Only a few patients will become litigants, but many others will just walk away vowing never to return to your clinic, and make sure that their friends and colleagues don’t either.
Unhappy patients demand your undivided attention, deplete your energy, and undermine the enthusiasm of your staff. To minimise the stress on the whole clinic, assign one staff member to follow the patient and foster a relationship of trust and confidence. Patients tend to confide more in non-threatening, empathetic ‘patient advocates’, than in the practitioner directly. It will only serve to instill more hostility in a dissatisfied patient to have to explain her problem to a different person every time she calls the clinic. Calls from unhappy patients should be handled immediately, rather than waiting for the patient to call back 2 hours later in an enraged state because no one in the clinic wanted to deal with him/her.
The importance of documentation
Meticulous documentation in patients’ charts will serve as your best defence when patients voice complaints. Even non-surgical treatments are not to be confused with non-medical treatments, and should only be performed in appropriate facilities under the supervision of a health professional who has been properly trained and is qualified to perform the procedure. In all cases, the patient’s chart should include an adequate medical history before any procedure or treatment is undertaken. Informed consent refers to adequately explaining potential risks, complications, and alternative treatments.
Medical procedures require sanitary surroundings and sterile instruments, as well as authentic equipment and medications. Even non-surgical procedures may occasionally result in unforeseen consequences; therefore clinics should have plans in place to handle every potential situation that may arise. Follow-up care is an important component of the doctor–patient relationship to ensure optimum results and a pristine patient experience.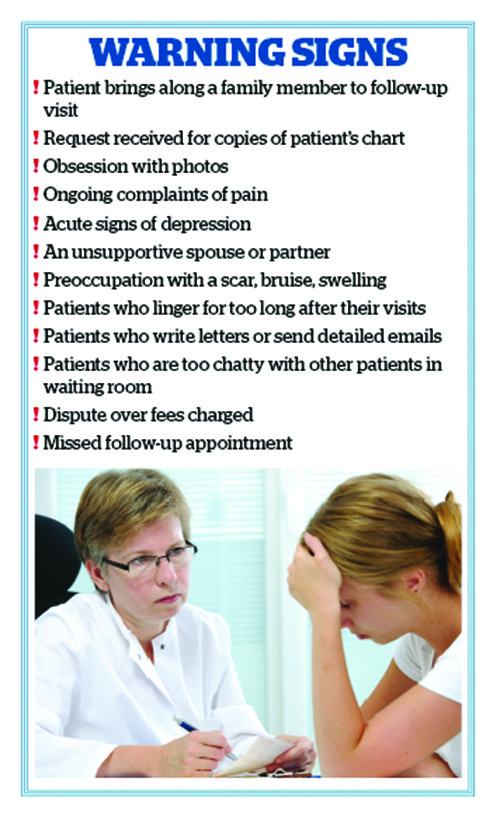
It is clearly best not to wait until the relationship between a patient and the clinic begins to break down to start documenting. Keep copious notes of all conversations, missed appointments, and non-compliant behaviour. Bring unhappy patients in for checks weekly, then monthly, then at 3 months, 6 months, and 12 months or more. Have a staff member accompany you at each visit and keep a running checklist of their complaints at every interval. As we all know, many of these problems will resolve without intervention by the next visit, or the patient will be less fixated on them as time goes on. If they miss a scheduled appointment, a letter may be sent for the purposes of documentation, and the clinic should also call the patient to reschedule. Maintain a dialogue with the patient during the initial period to demonstrate an interest in the outcome.
Keep in mind the statute of limitations where you practice and proceed accordingly. Courts take different views on when the statute of limitations begins. For example, in the state of California, actions against healthcare providers must be filed within 3 years after the date of the injury or 1 year after the plaintiff discovers, or should have discovered, the injury, whichever occurs first. Whereas in the state of New York, it is 2 years 6 months. In the UK, action must be taken within 3 years of the injury becoming known.
It is a fact of life in every cosmetic practice that sometimes revisions or additional therapies will be necessary; however, there is no standard guideline to follow. The time to cover the issue of the possibility of needing additional treatments is before the first. The patient should be informed before being treated of the possibility that a second procedure will be needed, and of what costs, if any, will be considered the patient’s responsibility. This can be written into the fee quotation form, signed by the patient, and kept on file. Unexpected expenses can do irrevocable damage to an already fragile doctor–patient relationship.
