Daniel Sister describes the beneficial use of carbon dioxide in improving aesthetic results and speeding up recovery time
Carbon dioxide is made up of one carbon atom (C) and two oxygen atoms (O), O-C-O, hence CO2. All humans and animals produce it during respiration as well as plants and trees via photosynthesis, which aids their growth.
Carbon dioxide is an odourless, invisible gas first discovered in 1648 (by Van Helmont) and Boyle described its anti-infective properties in the 17th century and by Lavoisier in the 18th century. Lalouette, in 1777, proposed the serial application of CO2 for treatment of chronic skin ulcers in the lower limbs.
Further beneficial health benefits of carbon dioxide were discovered in France in the 1930s when it was noted that bathing in the pools of carbon dioxide-rich water at the Royat Spas helped speed up wound healing.
In 1953 a group of cardiologists ascribed to the hospital of Clermont Ferrand, used this therapy in patients with illnesses related to poor blood circulation, fat accumulation and peripheric organic and functional arteriopathies and Jean Baptiste Romuef M.D. published a paper about his 20 years of experience in the subcutaneous injection of CO2.
Carbon dioxide has vasodilatory properties that make it useful to the medical community. The dilation of blood vessels leads to a decrease in blood pressure and a better flow of oxygen-rich blood around the body1.
How does carboxytherapy work?
All cells in the body, regardless of their role, release carbon dioxide as a waste product. Carbon dioxide is the ‘cost of doing business’ of any cell.
Whenever we breathe in oxygen, it is picked up by red blood cells. Each red blood cell carries four oxygen molecules, which it takes from the lungs to the heart via the blood vessels and then into the arteries and on a journey around the body to where they’re needed.
Whenever they encounter an area with high levels of carbon dioxide (which has been created by cellular metabolism), the red blood cells release oxygen molecules and pick up the carbon dioxide that they have produced.
Carboxytherapy is said to work by tricking the body, this works by injecting a small amount of carbon dioxide gas into the area, it will increase the dispatch of oxygen-laden red blood cells to the area to pick up the new ‘waste’ carbon dioxide that the body will then naturally eliminate via the lungs.
By increasing the amount of oxygen getting to the area, cells will become more active and thus speed up any healing or new cell production required to rejuvenate the area.
Physiology: the Bohr effect
Carbon dioxide helps the release of oxygen from haemoglobin and, as a result, the pH decreases, allowing the tissue to obtain enough oxygen to meet its demands.
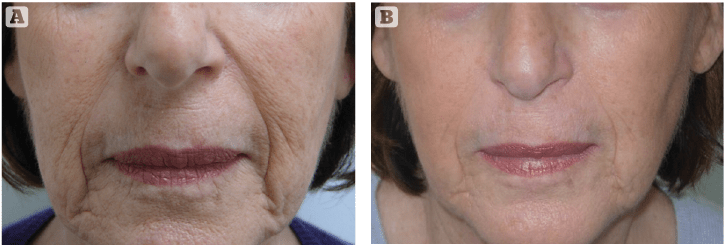
Figure 1 Nasolabial folds and marionette lines on the face (A) before, and (B) after treated with 12 sessions of carboxytherapy, twice a week for the first 3 weeks and then once weekly for 6 more weeks.
It is demonstrated by comparing the oxygen dissociation curves when there is less carbon dioxide present and when there is more carbon dioxide in the blood.
When carbon dioxide, in the presence of the catalyst carbonic anhydrase, diffuses into the blood plasma and erythrocytes, most of it reacts with water and the following dynamic equilibrium is established: H2O + CO2 = H2CO3.
Carbonic acid (H2CO3) dissociates to form hydrogen ions and hydrogen carbonate ions. H2CO3 = H+ + HCO3–
The negatively charged HCO3– ions, inside the erythrocytes, diffuse from the cytoplasm to the plasma. This is balanced by diffusion of chloride ions (Cl-) in the opposite direction, maintaining the balance of negative and positive ions either side.
The dissociation of carbonic acid increases the acidity of the blood (decreases its pH). Hydrogen ions (H+) then react with oxy-haemoglobin to release bound oxygen and reduce the acidity of the blood. Hb.4O2 + H+ = HHb+ + 4O2. It is this reversible reaction that accounts for the Bohr effect.
What happens during carboxytherapy treatment?
Carboxytherapy is similar to mesotherapy (a series of small injections with a thin needle), but it delivers medical grade carbon dioxide gas in a controlled flow/dose below the skin’s surface, rather than tiny quantities of a liquid formulation2,3.
Side-effects and contraindications
During treatment, some patients may feel slight discomfort, pressure or a stinging sensation as the gas is delivered to the tissues, (often described as a crackling sensation) as well as ecchymoses. Other side-effects can include minor swelling, redness (caused by the vasodilation), lasting anywhere from 1–5 days depending on the area treated. In the case of cellulite treatment, a warm sensation can be felt in the region for up to 24 hours.
Major adverse events are uncommon. In gynaecological laparoscopic surgery, large amounts of CO2 are used to expand the abdominal cavity (up to 4 litres of CO2) without any toxic effect.
At rest, with normal ventilation, the human body consumes 250 mL/min of oxygen (transported from the lungs to tissues) and exhales 200 mL/min of CO2 (removed from tissues and excreted through pulmonary alveoli).
In the case of hyperventilation, oxygen consumption can increase up to 4000–5000 ml/minute, and CO2 can increase to 4000–4500 ml/minute.
 During carboxytherapy an average of 30–50 ml/min CO2 are administered per session: the mild increase in CO2 levels are easily and, therefore, promptly resolvable by mild hyperventilation at the end of treatment, without risk of hypercapnia and respiratory acidosis.
During carboxytherapy an average of 30–50 ml/min CO2 are administered per session: the mild increase in CO2 levels are easily and, therefore, promptly resolvable by mild hyperventilation at the end of treatment, without risk of hypercapnia and respiratory acidosis.
Hypercapnia occurs when the lungs are unable to excrete CO2 and, therefore, pCO2 (partial pressure of carbon dioxide) significantly increases at the alveoli level. When the alveolar pCO2 reaches 60–75 mmHg, the patient can experience severe dyspnoea.
With a further increase to the pCO2 up to 80–100mmHg, the patient may become drowsy and lethargic (hypercapnic coma). With pCO2 alveolar levels of 120–150 mmHg, the excessive CO2 dampens the respiratory bulbar centre.
In normal conditions (healthy patients), there is no possibility to cause severe hypercapnia by carboxytherapy.
The primary excretion of CO2 and protons (H+) is performed by the kidneys and lungs. Severe damage to these organs (renal or respiratory failure) may lead to an excessive accumulation of CO2. In congestive heart failure, vessel circulation markedly slows down, and, consequently, the amount of CO2 removed from tissues is significantly lowered. Chronic congestive heart failure is another pathophysiologic condition causing CO2 accumulation in which using carboxytherapy is questionable.
Carboxytherapy should also be avoided in patients under treatment with carbonic anhydrase inhibitors (acetazolamide, diclofenamide). As the use of the inhibitor obstructs the primary process by which CO2 can be excreted through the lungs and kidneys.
Severe anaemia implies a significant decrease in red blood cell numbers, which is a substantial decline in the availability of the leading carrier by which CO2 can be usually transferred to the lungs and kidneys to be eliminated. Severe anaemia also signifies a decrease in haemoglobin levels, and this reduces the possibility of CO2 binding to form carbaminohaemoglobin, the second most relevant CO2 carrier from tissues to lungs and kidneys.
A decrease in plasmatic protein levels may be caused by chronic liver insufficiency that constitutes another contraindication for carboxytherapy. Another contraindication is the presence of gaseous gangrene. This severe infectious disease is caused by anaerobic bacteria entered in the body through skin wounds and is characterised by extensive tissue damage, necrosis, oedema and severe generalised deteriorated conditions.
Indications and clinical data
The most common aesthetic uses of carboxytherapy are for treating cellulite, fat reduction, striae (stretch marks), acne scarring, skin laxity, dark circles under the eyes and wrinkle reduction. Therefore treatments are generally focussed on the face, neck, arms, abdomen, and thighs4.
In 2001, the University of Siena (Italy) investigated CO2 treatment of localised fat deposits on the thighs, knees and/or abdomen in 48 women. The CO2 was administered via subcutaneous injections twice weekly for 3 weeks (equalling a total of 6 treatment sessions)5.
The results showed that on average, the women lost 2 cms of circumference from their thighs, 1 cm from the knees, and almost 3 cms from the abdomen. The skin in the treated areas also appeared thicker than before treatment, with cellulite appearing smoother. Few minor side-effects were observed but all resolved very quickly.
In 2004 the same university published another study looking at the effects of carbon dioxide on skin irregularity and its use as a complement to liposuction. Forty-two patients treated for fatty tissue accumulations on the thighs and knees were divided into three groups. In group 1, only liposuction was performed; in the second group, carboxytherapy was administered 3 weeks after liposuction in twice-weekly applications for 10 consecutive weeks; and in the third group, carboxytherapy alone was delivered, again twice-weekly, for 10 consecutive weeks6.
The results were then analysed by reporting on variations in circumference measurements and skin elasticity after 2 months. The authors noted that liposuction alone did not generally have a positive enough effect on skin irregularity and could, in fact, cause uneven areas; however, the addition of carboxytherapy provided an improvement in skin smoothness and elasticity. Carbon dioxide therapy also showed positive results in reducing fat accumulation as the circumferential measurement results of those treated with liposuction and carbon dioxide were better than for those treated with liposuction alone.
In March 2008, a Brazilian study looked at whether the intradermal and subcutaneous injection of carbon dioxide into the skin of rats would increase the turnover of collagen. Following biopsies, it was noted that collagen turnover had increased compared to the control animals (which were injected with only saline) and that the collagen formations were more pronounced in the areas where the gas was injected intradermally, as compared to where it was injected subcutaneously7.
Improved adiposity through lipolysis
The effects of CO2 therapy lipolysis include:
- Fracturing of the adipose tissue
- Release of triglycerides in the intercellular spaces
- Adipocytes present thin fracture lines in the plasma membrane. These lines did not involve the connective spaces where the major vascular structures are located4,8.
Brandi C et al. wrote in his study: ‘Carbon dioxide therapy in the treatment of localised adiposities: clinical study and histopathological correlations’, published in Aesthetic Plast Surgery, ‘The data regarding measurements of the maximum circumference of the thigh, knee, and abdomen taken before and at the end of the study showed a significant reduction in all patients.’4
At the injection site, the CO2 gas penetrates and spreads to other tissue nearby, and keeps on doing its work liberating bradykinin, serotonin, histamine, and catecholamine, which stimulate the beta-adrenergic receptors, producing lipolysis (destruction of fat cells)9,10.
 When the CO2 comes in contact with fat, it diffuses, with part of it going to red blood cells. This is where it attaches to the haemoglobin and sends oxygen to the tissue, which then permits metabolic reactions.
When the CO2 comes in contact with fat, it diffuses, with part of it going to red blood cells. This is where it attaches to the haemoglobin and sends oxygen to the tissue, which then permits metabolic reactions.
Carboxytherapy works in three complementary ways. First, carbon dioxide mechanically kills fat cells by breaking off their membranes. Second, it has a strong vasodilatory effect (causes dilation of blood vessels) on the capillaries in the area. It also increases the percentage of oxygen in the tissue. Wider vessels mean bigger and stronger blood flow to the area. The increase in oxygen is important because it eliminates the built-up fluid from between the cells. And thirdly, it improves the cutaneous elasticity and induces a rejuvenation of the dermis.
Carboxytherapy is generally cheaper for patients than a course of Endermologie®, Smartlipo®, Ultrashape®, Velasmooth®, Thermage®, Accent® or Coolsculpt®, plus it’s a much cheaper investment for your clinic in terms of equipment, clinical environment, insurance and per patient accessories. It is also much easier to transport from clinic to clinic, and there is almost no risk for the patient.
Dark circles under the eyes
One of the major causes of dark circles under the eyes is vascular pooling. The capillary network under the lower eyelids can become congested for a number of reasons. Normally tears drain from the eyelids into the nose, but if there is an obstruction due to chronic nasal congestion from seasonal allergies, previous nasal fracture, or a deviated septum, the drainage doesn’t function well, and the blood flow to the lower eyelids becomes sluggish, giving rise to a boggy blue tinge.
The lack of oxygenation to lower eyelid skin allows the bluish cast to show through the thin skin. Carboxytherapy works to improve the capillary network of the lower eyelids, as well as to increase the dermal collagen layer in the lower eyelid skin. By injecting a small amount of carbon dioxide gas into the affected areas, blood flow is increased and improved capillary networks are formed. The bluish cast is replaced with a healthy pink tone. Once a series of treatments have been completed, the skin has a more luminous appearance that lasts approximately 6 months10,11.
Stretch marks
When treating stretch marks, note that studies show a better response to treatment when the marks are recent, and still red in colour, rather than when they are older with a more faded, silvery appearance. Newer stretch marks will most likely require treatment once a week for 2–4 weeks, although in some cases (depending on severity) a single session is enough. Older stretch marks will need 3 or 4 treatment sessions at 3–4 weekly intervals12-14.
Cellulite
Cellulite is partly a circulatory disorder at a local level. When drainage of fat cells does not occur, waste and impurities build up15–20.
Cellulite is the result of a number of biochemical and metabolic alterations which all begin in the interstitial matrix and on connective structure levels, these include:
- PH alterations (acidity levels)
- Free radical increase
- Temperature alterations
- Oxydo-reduction alterations
- Lymphatic stasis.
The glucosaminoglycans (GAG) are responsible for the movement of blood in a microcirculation. When GAG is reduced, there is also a decrease in the movement of the microcirculation, with less blood circulating and an alteration in the form of the fat cells, oedema, and fibrosis can occur.
The accumulation of this thick liquid produces irritation in the fibroblasts. They start to produce collagen in larger volumes; as a result, there is traction in the dermis, which causes the ‘orange peel’ look.
When CO2 is injected in the affected area, the situation is reversed. Vessel dilatation occurs and the speed of the microcirculation improves. The tissue receives more oxygen, toxins are eliminated, and the oedema reduces.
Through the therapeutical effects mentioned before, it re-establishes the morphology and functionality of the microcirculation; by raising the quantity and speed of the blood flow, diminishing the accumulation of liquids between the cells, disintegrating the fat of the hypodermis, and diminishing the fibrosis. In a few weeks, natural local metabolism is stimulated, due to the increase in the microcirculation, the elimination of toxins, and the activation of the lipolysis process (destruction of the adipose tissue).
Conclusion
New equipment makes carboxytherapy a very easy to perform, cheap, and versatile option to treat multiple and various skin conditions. From vascular disease to dark circles under the eyes. From cellulite to fat deposits. From psoriasis to stretch marks and scars21–25.
Declaration of interest None
Opening image © Shutterstock
Figure 1 © Dr Sister