


Gabriela Casabona shares her seven-step approach to treat skin laxity and restore volume to the neck

Neck rejuvenation is a common request from patients seeking to improve their appearance. It has been well documented how impactful aesthetic procedures can be on a patient’s lifestyle and self-esteem.1 Among the patients seeking non-surgical procedures in our clinic over the last 5 years, 30% were requesting neck rejuvenation, specifically. Many patients seeking neck rejuvenation believe that the problem is at the skin level; however, the neck is impacted by ageing across the neck and other regions, such as the mandible, mid-face, and temples2,3. Therefore, planning treatments to rejuvenate the neck becomes difficult. The solution lies in using combinational procedures not only to address the problem in the neck region but in the other regions as well4.
Understanding the ageing process across each layer, such as the superficial musculoaponeurotic system (SMAS), skin, and fat, is vital to correctly evaluate and determine a treatment plan when considering the use of energy-based devices, threads, biostimulation or fillers.
In 2019, a study5 performed on 200 patients evaluated the ageing of the SMAS as well as the superficial and deep fat layers in different age groups, gender, and body mass index (BMI). While in 2022, another group looked into the same age groups, gender and BMI but included the skin thickness6. Both studies concluded that with age, the SMAS became more superficial in certain areas, such as the preauricular, submandibular, and neck due to the loss of the superficial fat layer. In addition, there was evident thinning of the skin, especially in the neck, related to the patient’s age. Therefore, with a patient who is over 45 and seeking neck rejuvenation, it is likely I will have to address skin thickening as well as add support to the skin below the dermis by adding or restoring the fat layer. I may choose to combine PRP and microneedling7 or radiofrequency to treat the skin surface plus HA or biostimulators to restore the subdermal layer.
The patient’s anatomy must assume an important role when deciding on the treatment protocol. In 2019 Casabona et al.8, highlighted the importance of treating the lateral face first. In 2020, the same group9 revealed the effect of posterior temples on several areas of the face, demonstrating that by adding support to the lateral face, the amount of product needed to treat the medial face decreases. The neck is no different. Treatments conducted on the posterior temples9 and lateral face impact the lower face6, or more precisely in the mandible area, as much as treatments in the chin area also improve the submandibular region10.
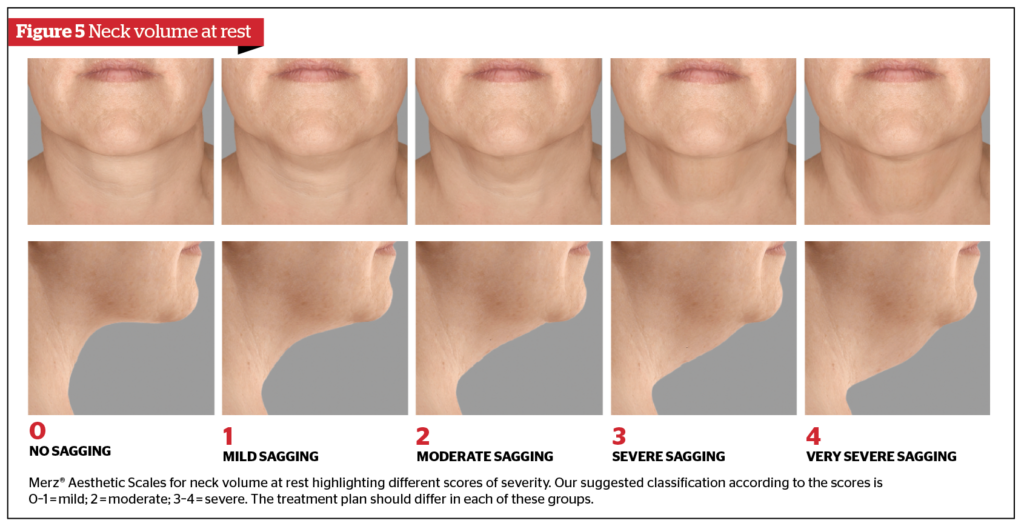
From the patients that presented in our practice over the past 5 years for neck rejuvenation, we observed a clear pattern between those who were happy with their procedure and results. Using the Merz Aesthetics Scales™ score for the neck, it was clear those with a score of three (severe sagging) required treatment across more regions than a patient with a score of two (moderate sagging). In addition, the patient rated three on the scale required therapies across more layers and per area than a patient-rated two on the scale. Therefore, it is important to understand what the patient really wants, how comfortable they are with the post-procedure downtime, and how much they are willing to invest (in time and money) to get the desired result. Using the Merz Aesthetics Scales for neck volume and neck laxity can help create a visual aid and common ground of reference on what is ‘mild’ and what is ‘severe’ ageing in the region, as well as a guide on volume and laxity.
The seven step approach
In the last 5 years, we developed a systematic way of evaluating a patient’s condition so that our planning became more precise and we could better match the patient’s expectations. Considering that most patients have high expectations of either 3 or 2 point improvement in neck laxity or neck volume (Merz Aesthetics Scales), we developed seven steps to assess the patient and choose the correct techniques to be used in combination:
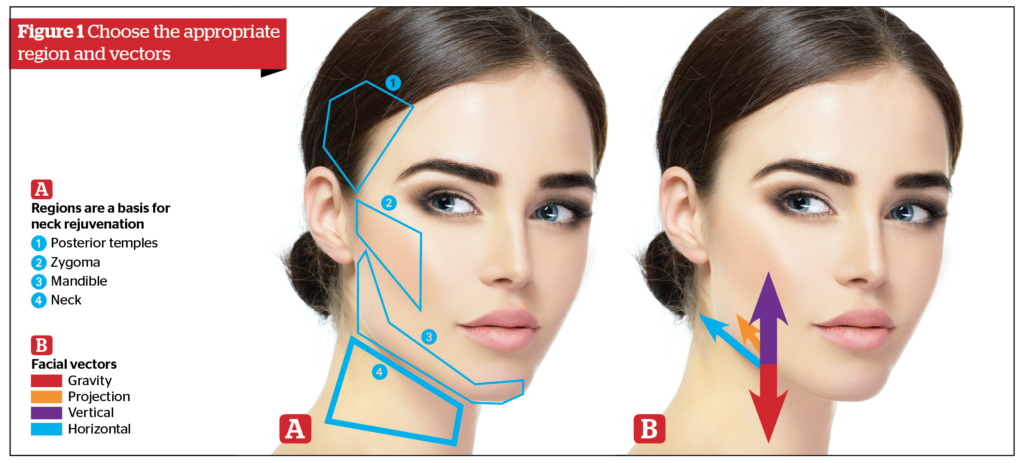
Step 1: Choose the appropriate regions to treat. A general rule is the more severe the ageing, the more areas involved (Figure 1). Also, it is very important to consider individual patient anatomy to understand how the regions in the neck and face impact one another8,9. For example, the treatment of the zygoma area has a significant effect on the mandible area; the same is true of injections to the posterior temples, which impact the lateral face, zygoma, and mandible, thereby impacting the upper neck.
Step 2: Choose the appropriate vectors. As ageing progresses, the loss of bone, fat, and skin thickness have an impact on the vectors in the face and neck. For lower face and neck rejuvenation, the vertical and horizontal are more important than the projection (Figure 1B). Specifically for the neck, the vertical vector means either to enhance the vertical height of the mandible or to shorten structures, such as the SMAS (platysma and fascia) from the mandible to the clavicle11. While addressing the horizontal vectors would require creating some shortening in the direction of the back of the neck by strengthening the SMAS. The only projection vector that can interfere with the neck is the chin or masseter width enhancement, but this can only be performed in a few individuals.
Step 3: Identify the problematic layer, be it bone, fat, muscle, fascia or skin.
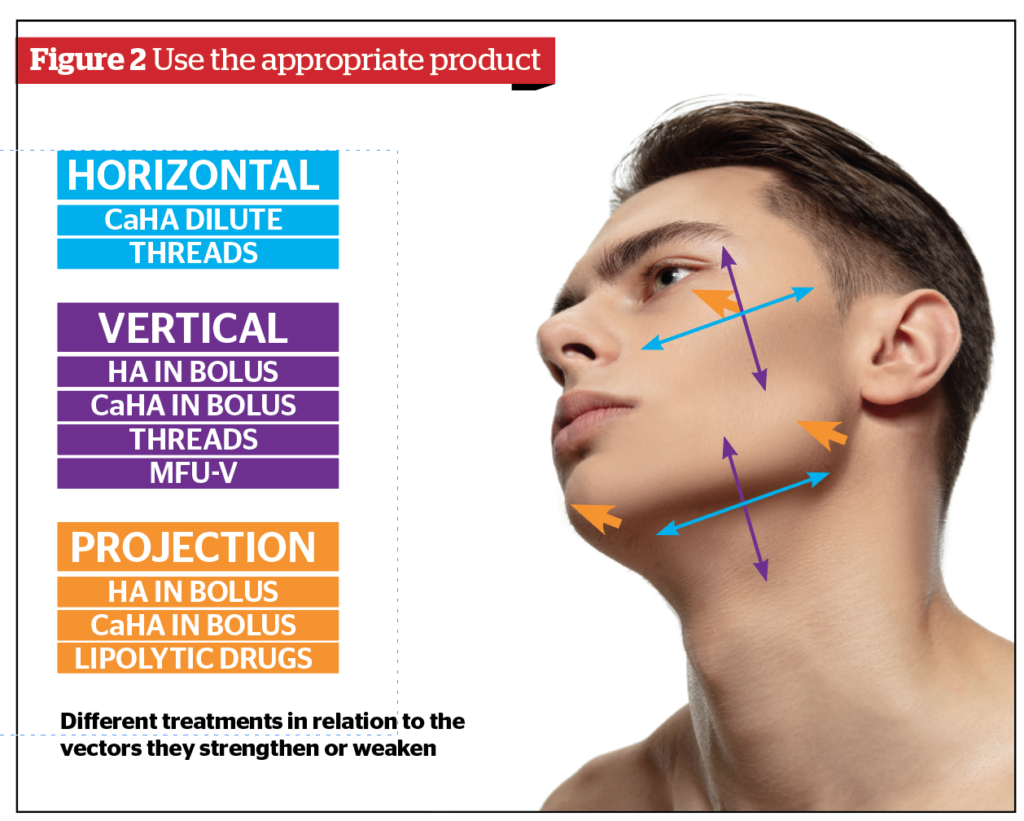
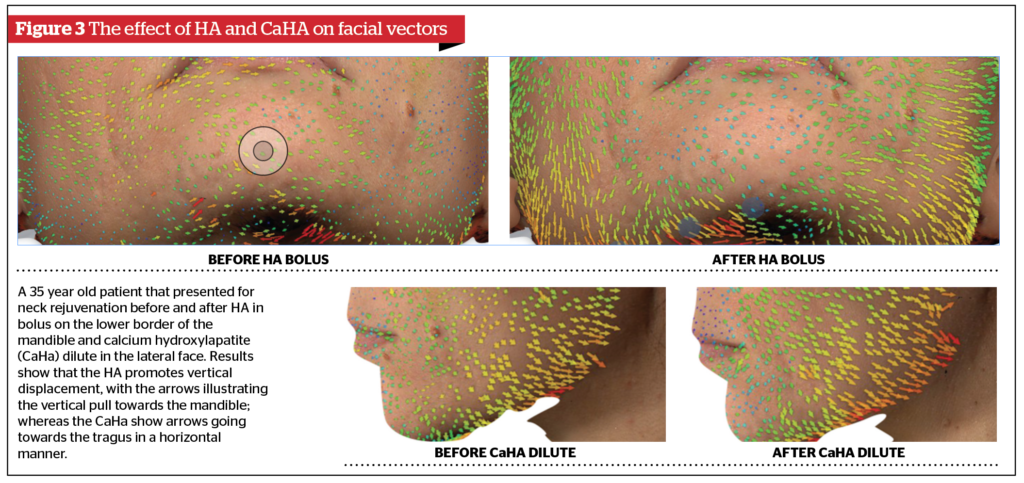
Step 4: Choose the treatment according to the vectors. Every procedure we do strengthens or weakens a particular vector against gravity. If you use a bolus of HA in the zygoma area, we strengthen the projection effect. In contrast, if you inject CaHA dilute in the lateral face, you strengthen the horizontal vector of the face, or if you inject the same HA in the lower border of the mandible, you strengthen the vertical vector (Figure 2–3).
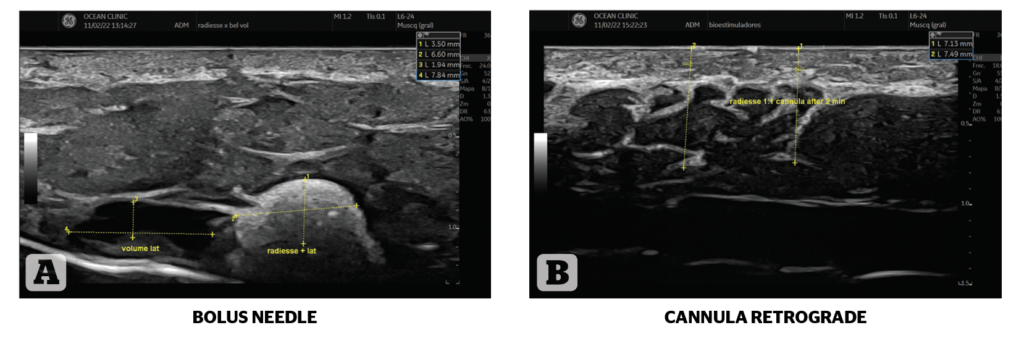
Step 5: Choose the layer to treat according to the best use of the product. Perhaps a product has a better projection capacity if used deep in the supraperiosteal area instead of subdermal. Consider too how you deliver the product, as both a bolus and retrograde technique may convey a unique projection capacity (Figure 4).
Step 6: Choose the amount of product to use depending on the severity of ageing (Figure 5).
Step 7: Select a maintenance plan depending on the severity of ageing. Once we have completed our step-by-step treatment approach, the essential next step is to follow up with our patients to maintain the results and prevent any complications12. Depending on the procedure, a specific time frame should be respected for immediate and long-term follow-up.
For example, filler injections should be followed up the next day with a text or call asking about any lumpiness, pain, bruising or discolouration to ensure there are no complications. On the other hand, there is no sense in following up following a toxin injection after one day; this should happen around day 15, as this is when we see tend to witness the major complications, such as ptosis, asymmetries and lack of any satisfactory result.

Conclusion
Treating the neck can be very complex as two patients seeking neck rejuvenation can have varying degrees of ageing severity, different goals, and different layers involved, the plan and treatment combinations need to be entirely distinct; illustrating how complicated and tricky the decisions for neck rejuvenation can be.
In conclusion, it is essential to be systematic not only in the evaluation of the neck but also when choosing procedures, as each decision can make a difference in the amount of product to be used and the time it will take to get the desired result.
Declaration of interest The author is a consultant and KOL for Merz Aesthetic
Figures 1–6 © Dr Casabona
References
- Cohen JL, Rivkin A, Dayan S, Shamban A, Werschler WP, Teller CF, Kaminer MS, Sykes JM, Weinkle SH, Garcia JK. Multimodal Facial Aesthetic Treatment on the Appearance of Aging, Social Confidence, and Psychological Well-being: HARMONY Study. Aesthet Surg J. 2022 Jan 12;42(2):NP115-NP124. doi: 10.1093/asj/sjab114. PMID: 33751048; PMCID: PMC8756087.
- Friedman O, Shamban A, Fabi S, Duncan DI, Artzi O. The Aging neck-A Case base treatment algorithm. J Cosmet Dermatol. 2021 Feb;20(2):569-576. doi: 10.1111/jocd.13877. Epub 2020 Dec 19. PMID: 33340202
- Casabona G, Kaye K. Facial Skin Tightening With Microfocused Ultrasound and Dermal Fillers: Considerations for Patient Selection and Outcomes. J Drugs Dermatol. 2019 Nov 1;18(11):1075-1082. PMID: 31738490.
- Pérez P, Hohman MH. Neck Rejuvenation. 2022 Feb 27. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan–. PMID: 32965900.
- Casabona G, Frank K, Koban KC, Schenck TL, Lopez VP, Webb KL, Hamade H, Freytag DL, Green JB, Cotofana S. Influence of Age, Sex, and Body Mass Index on the Depth of the Superficial Fascia in the Face and Neck. Dermatol Surg. 2019 Nov;45(11):1365-1373. doi: 10.1097/DSS.0000000000001909. PMID: 30882511.
- Kwon SH, Ahn GY, Lew BL, Shin JW, Na JI, Huh CH. Clinical Implication of the Regional Thickness of the Lower Facial Skin, Superficial Fat, and Superficial Musculoaponeurotic System on High-Intensity Focused Ultrasound Treatment. Dermatol Surg. 2022 May 1;48(5):527-531. doi: 10.1097/DSS.0000000000003393. Epub 2022 Jan 26. PMID: 35093961.
- Gawdat H, Allam RSHM, Hegazy R, Sameh B, Ragab N. Comparison of the efficacy of Fractional Radiofrequency Microneedling alone and in combination with platelet-rich plasma in neck rejuvenation: a clinical and optical coherence tomography study. J Cosmet Dermatol. 2022 May;21(5):2038-2045. doi: 10.1111/jocd.14331. Epub 2021 Jul 10. PMID: 34214220.
- Casabona G, Frank K, Koban KC, Freytag DL, Schenck TL, Lachman N, Green JB, Toni S, Rudolph C, Cotofana S. Lifting vs volumizing-The difference in facial minimally invasive procedures when respecting the line of ligaments. J Cosmet Dermatol. 2019 Aug 12. doi: 10.1111/jocd.13089. Epub ahead of print. PMID: 31402563.
- Casabona G, Frank K, Moellhoff N, Gavril DL, Swift A, Freytag DL, Kaiser A, Green JB, Nikolis A, Cotofana S. Full-face effects of temporal volumizing and temporal lifting techniques. J Cosmet Dermatol. 2020 Nov;19(11):2830-2837. doi: 10.1111/jocd.13728. Epub 2020 Oct 5. PMID: 32946624.
- Vanaman Wilson MJ, Jones IT, Butterwick K, Fabi SG. Role of Nonsurgical Chin Augmentation in Full Face Rejuvenation: A Review and Our Experience. Dermatol Surg. 2018 Jul;44(7):985-993. doi: 10.1097/DSS.0000000000001461. PMID: 29309340.
- Gentile RD. Renuvion RF-Helium Plasma for Subdermal Skin Tightening, Facial Contouring and Skin Rejuvenation of the Face and Neck. Facial Plast Surg Aesthet Med. 2020 Jul/Aug;22(4):304-306. doi: 10.1089/fpsam.2020.0070. Epub 2020 May 5. PMID: 32379988; PMCID: PMC7374633
- Truswell WH. Complications in Lower Face Rejuvenation: Avoiding, Minimizing, Recognizing, Dealing with Them, and Helping the Patient through the Process of Fixing the Problems. Facial Plast Surg. 2020 Aug;36(4):462-477. doi: 10.1055/s-0040-1713823. Epub 2020 Aug 31. PMID: 32866983.



{kind=link}