



Amy Miller looks at the use of dermal fillers as an alternative to surgical methods to rhinoplasty, including techniques, products and complications
Until the advent of injectable tissue augmentation with dermal filler, the shaping of the nose was strictly the domain of the plastic surgeon. The only way to effectively change the size or contours of the nose was to go to the O.R., anaesthetise the patient and use a scalpel. Subsequent oedema could then sometimes cause distortion and even graft failure or other issues, regardless of the impeccable technique employed by the surgeon. Even the best surgeons have experienced contractions and rotational deformities post-surgery and injectable products can be useful tools for post-surgery complications1. In these cases, many surgeons used medical grade silicone, off label, for fine-tuning of the surgical results. With the addition of many types of safe, temporary, dermal fillers to the market, many patients can ‘try out’ a nose treatment before going to surgery, or avoid surgery altogether. Surgical rhinoplasty will always be the gold standard for certain nasal deformities, but non-surgical rhinoplasty (NSR) has become a viable, less aggressive, option for many patients.
Non-surgical rhinoplasty is often called injectable rhinoplasty or medical rhinoplasty in the literature. For consistency and simplicity it will be referred to as non-surgical rhinoplasty or NSR in this article. Patients that are candidates for NSR include: those who cannot or will not have a surgical procedure; those that have cartilage irregularities that can be disguised with filler; those that have a low radix giving the illusion of a ‘short’ nose; those with certain polly beak or saddle deformities of the dorsum; and those with a droopy nasal tip. Additionally, patients that want minimal downtime and cost may be NSR candidates. Any patients that have a large, protuberant nose or protuberant ‘humps or bumps’ will require surgical rhinoplasty. Reduction rhinoplasties are only obtainable with surgery.
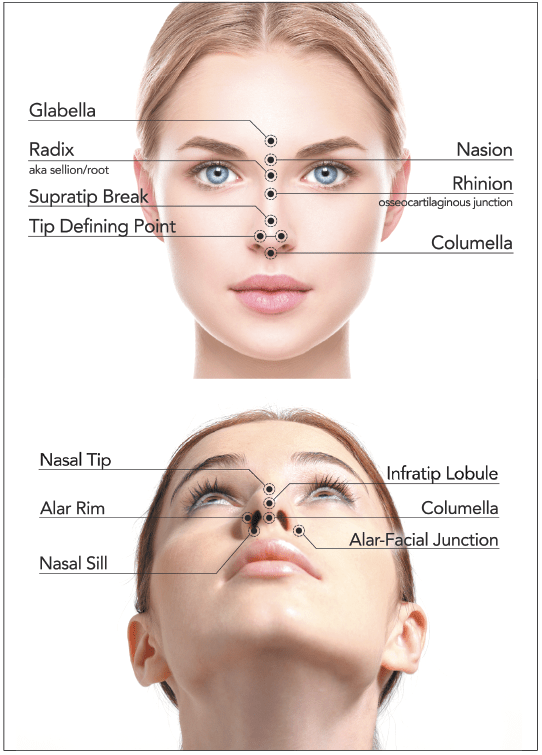
Figure 1 Surface nasal anatomy
As with any procedure, there are risks and benefits. While patients may be motivated by the many perceived benefits, he or she must be informed that NSR is not without risks. Vascular occlusion by the dermal filler product is the most feared, with all its subsequent problems, such as tissue necrosis and blindness. Other, more plebian issues, such as infections, Tyndall effect, nodule formation and biofilms are possible and need to be recognised when they occur. Additionally, it is essential to be aware that the post-surgery nose has a higher risk of complication with NSR due to altered anatomy and blood supply, so extra caution must be taken and the presence of a graft of any sort should be looked at as a contraindication in most patients2.
Nasal anatomy
It is imperative to have a solid working knowledge of the nasal anatomy not only for treatment purposes but for communication purposes as well. Common landmarks on the nose include the: radix/sellion, nasion, rhinion, tip defining points, infratip lobule, supratip break, columella and ala (Figure 1A and 1B).
The nose is an integral part of the aesthetic balance of the face. Because it occupies the centre of the face, mild asymmetries can be quite striking3. Noses that break the rules of thirds and fifths of the face, as well as the phi ratio or ‘golden rule’ can be jarring as well. Ideally, the nose, from the tip to radix, should occupy the middle horizontal third of the face, and from nare to nare should span the width of the centre vertical fifth of the face (Figure 2). The Phi ratio, also referred to as the Fibonacci sequence or golden ratio, is a mathematical expression that attempts to measure beauty. The ideal ratio is 1:1.6. For example, if the width of the face is 1.0, the height should be 1.6. The nose is also subject to this Phi ratio. If the length of the bridge of the nose, from tip to cartilaginous boney junction is one, the length from tip to root should be 1.6. Nasal deviations from this golden ratio can disrupt the harmony of the facial features. Often the ratios can be improved with NSR.
The nasal architecture also contributes to two important facial measurements, the nasofrontal angle and the nasolabial angle (Figure 3). Alterations to the nose can change the degrees of these angles and these changes need to be considered before any surgical or non-surgical nasal reconstruction is performed. A satisfactory aesthetic result for the nasolabial angle is considered between 90 and 100 degrees for men and 95 to 110 degrees for women4. Therefore, the ideal female nose is more raised than the male nose5. Sometimes this angle can be slightly widened by a small dose of neurotoxin. The muscles that rotate the nasal tip towards the maxillary bone are the depressor septi nasi and levator labii alaeque nasi and they can be accessed relatively easily for treatment with a neurotoxin6.
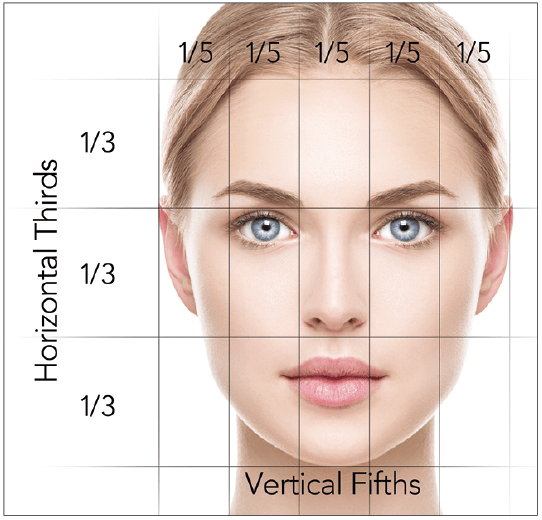
Figure 2 Facial thirds and fifths
The nasofrontal angle should be around 130 degrees. A study from the UK published in 2016 found that a nasofrontal angle of 130 is considered ideal, with a range of 127 to 142 degrees deemed acceptable7. These authors also found that angles above or below this range were perceived as unattractive and anything outside the range 118 to 145 was deemed very unattractive7. The best patients to treat with NSR are patients with an angle that is too deep8; in other words, less than 130 degrees. This angle is altered by adding filler to the dorsum and radix and will be discussed in more detail later.
Knowledge of the arterial supply of the nose is of utmost importance when contemplating NSR (Figure 4). The dorsal nasal artery often anastomoses with the supratrochlear artery, which then feeds into the ophthalmic artery. Needless to say, an embolus to the ophthalmic artery could be disastrous. The lateral nasal artery is a branch of the facial artery that supplies the nasal alae and
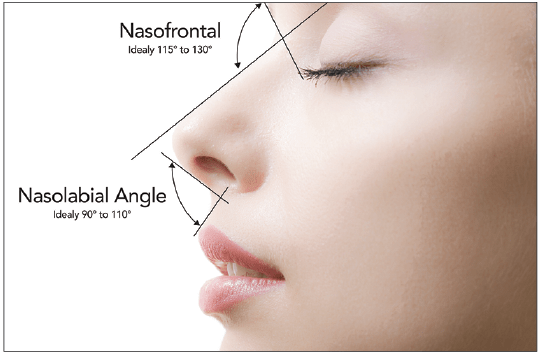
Figure 3 The nasofrontal and nasolabial angles
communicates with the dorsal nasal artery to supply the tip9. Collateralization in the ala is poor, so a compromise of the lateral nasal artery or its alar branch may lead to necrosis10.
Compromise can occur not just from embolisation but from compression secondary to product and/or oedema as well.
It is essential to respect and support the cartilaginous and boney architecture of the nose during NSR (Figure 5). The junction of the nasal bone and the septal and lateral nasal cartilages is called the rhinion. It is at this point that many ‘humps’ or ‘dips’ occur that can be corrected with NSR. The supratip area is where the lateral cartilages meet the alar cartilage and can be the sight of ‘polly beak’ deformities. These deformities are either genetic or subsequent to surgical rhinoplasty11 and can often be camouflaged. Support to the columella, at the anterior nasal spine and between the medial crus of the alar cartilage can be helpful for projection.
Nasal nerves and anaesthesia
Knowledge of the innervation of the external nose can be useful when anaesthetising the area for injections. The ophthalmic and maxillary branches of the trigeminal nerve provide sensory innervation. The superior aspect of the nose is supplied by the supratrochlear and infratrochlear nerves, as well as the external nasal branch of the anterior ethmoidal nerve. The inferior and lateral parts are supplied by the infraorbital nerve12. Use of infratrochlear nerve block will help anaesthetise the radix area without distortion to the anatomy.
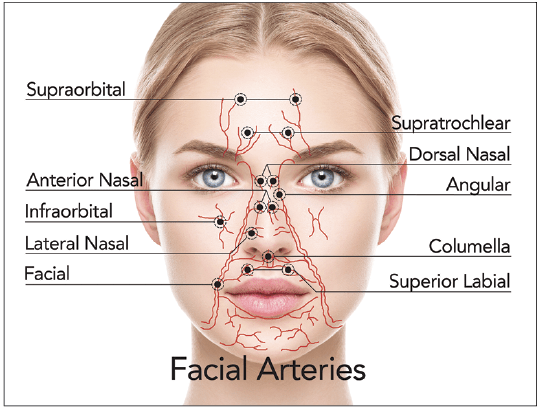
Figure 4 Blood supply to the nose
Similarly, an infraorbital block will numb the nares/ala area. Rather than blocking the entire infraorbital nerve, the medial branches can be anaesthetised by infiltrating along the frontal process of the maxilla, approximately along a line where a low lateral osteotomy would be performed9. The external nasal branch of the anterior ethmoidal nerve, which innervates the mid-dorsum, can be blocked via a nasociliary nerve block13. This is more technically demanding and may not be appropriate in the outpatient setting. Local infiltration is contraindicated because of the distortion to the tissues to be treated. For this area, topical anaesthetics are reasonably effective if the appropriate time interval elapses before injection14. Finally, if injections to the tip or columella are planned the anterior superior alveolar nerve can be blocked. This is done intraorally, with the local anaesthesia being injected at the anterior nasal spine (application of topical anaesthesia to the oral mucosa around the frenulum makes this more comfortable)9.
There is a debate regarding the use of epinephrine as a component of the injectable or topical anaesthesia in the setting of NSR. The addition of epinephrine has the benefit of local vascular constriction with less bruising and bleeding and a longer duration of anaesthesia. However, the local vasoconstriction and blanching can be difficult to distinguish from ischaemia and blood vessel compromise15. As early recognition of this most feared complication is essential, the benefit of epinephrine may be outweighed by the risks15.
Types of fillers for NSR
The most popular fillers for NSR tend to be hyaluronic acids and calcium hydroxyapatite. Both are naturally broken down by the body and, therefore, are not a permanent treatment. Hyaluronic acid has the added benefit of being reversible by hyaluronidase if an intra-arterial injection or other problems occur or even if the outcome is just less than desirable. Autologous fat, polymethylmethacrylate and silicone are other, albeit, less employed options. These can all be considered permanent to some degree. In the author’s opinion, the permanent fillers should only be used after both the patient and injector have had at least one ‘dress rehearsal’ with biodegradable filler.
When choosing which product to use for NSR, it is important to consider the rheological properties of the filler. The first is the elastic coefficient (G’), which measures the ability of the product to store mechanical energy and resist flow16 or resist deformation when pressure is applied to it9. In general, the G’ increases with the amount of crosslinking of the HA molecules and can be thought of as a measurement of the stiffness of the gel. Gels with higher G’ can resist dynamic forces better during facial muscle movement, thus providing better potential lift and duration for the filler17. However, these materials may be stiffer, lumpier and induce greater trauma with pain, inflammation and oedema as post-injection sequelae16. Lower G’ products tend to ‘blend’ more readily into surrounding tissue but may not be able to resist deformation forces as well as higher G’ products.
Just as important as G’ is the viscosity of the product or n*. Viscosity seems similar to G’ and indeed, scales with it, but more precisely n* refers to the ability of the gel to resist shearing forces18. Lower viscosity products are more easily spread and high n* products tend to stay put, making for more precise sculpting9. There is less diffusion into surrounding tissue and generally a more predictable result with higher viscosity fillers.
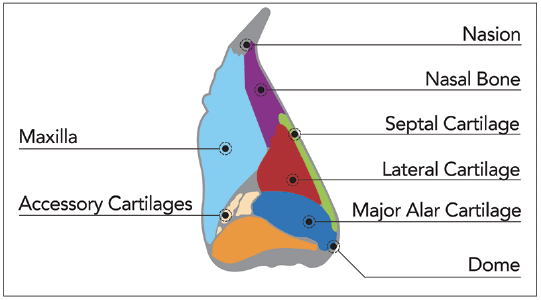
Figure 5 Nasal bone and cartilages
Next, a non-rheological property to consider when choosing filler is the hydrophilicity of the product. Native hyaluronic acid molecules bind enormous amounts of water and help to give the skin its supple, resilient quality19. Injectable hyaluronic acids bind water in a similar fashion, with different manufacturers manipulating this property for different applications. Therefore, the different HA’s on the market have variable water-binding abilities. In many cases, high hydrophilicity is considered a desirable effect, especially where a voluminous look is desired, such as in the lips. This, however, is usually not the case with the nose. Products that do not absorb much water are better for NSR as there is less tissue distortion and less chance of vascular compression secondary to oedema.
Finally, it is essential to keep in mind how the addition of lidocaine affects the flow, elasticity, and viscosity of the various fillers. Wang and Friedman report that the G’ and n* are directly proportional to material concentration and therefore, by decreasing the concentration by dilution with lidocaine, the injector can decrease G’ and n*. This allows for ‘customisation’ of the product for its intended purposes. A recent publication from Switzerland reiterates this concept. These authors found that adding lidocaine to a series of well established HA gels resulted in modification of the gels’ rheological properties. They found that these modifications occurred to a variable extent depending on the gel, as compared to the test results obtained when no lidocaine was added20.
An ideal filler for NSR would be minimally hydrophilic, have high G’ and n*, and be easily reversible. No currently available injectables meet all these criteria. Calcium hydroxyapatite comes closest, but it is not reversible. Nevertheless, it is the favoured product for NSR of many authors9, 15, 21. CaHA may have superior longevity21 when compared to the HA’s appropriate for nasal injection and this adds to its allure.
Autologous fat, polymethylmethacrylate and silicone are all options for long term to permanent NSR. Autologous fat, unlike the other options, is abundant and readily available22. Fat is harvested, centrifuged and prepared for injection. There is variability in the fat grafts’ ability to survive and there is inevitably some absorption, requiring repeat treatments. Various studies have reported a graft retention rate of 44.5%23 to < 50%24 after 1 to 3 treatments. Other studies measured good to high patient satisfaction rates of >80%25 but graft retention levels were not ascertained. This alludes to the fact that other factors contribute to patient satisfaction, not just the volume of fat survival and viability of the graft. This would be an interesting topic for further investigation.
Polymethylmethacrylate is a unique, long term, possibly permanent filler, consisting of PMMA microspheres suspended in bovine collagen. It has undergone several reformations in its lifetime to reach today’s product, Bellafill, marketed by Suneva.
In 2013, Rivkin reported it to be a safe and effective means to correct nasal contour irregularities26. A study from 2014, comparing Artecoll, an early form of Bellafill with less uniform PMMA particle sizes, with an HA product as well as silicone, found PMMA to be the superior filler16, 27. PMMA resulted in the least amount of side-effects and was able to maintain results 12 months post-procedure27.
Silicone has been used for several decades as a soft tissue filler in general and as a tool for post-surgical rhinoplasty revision. Medical grade silicone is marketed by Alcon and is FDA approved in the US for treatment of retinal detachment. It is frequently used off-label for cosmetic purposes21, but any use of dermal fillers in the nose is currently considered ‘off-label.’ A report from 1986, detailing silicone treatment to the nose in 347 post surgical rhinoplasty patients, found it to be safe, effective, and a valuable adjunct to cosmetic rhinoplastic procedures28.
Silicone has a reputation as being high risk for initiating a foreign body response from the body and inducement of granulomas16 and many practitioners are afraid to use it. It is important to keep in mind that many reports do not distinguish between medical grade silicone and industrial grade silicone. One example is a case report of cosmetic enhancement of the hip and buttocks via silicone injections, performed in a local hotel room by non-medical personnel resulting in disfiguring granulomas29. It is unclear how many of these problems are due to contaminated product or the illegal practice of medicine, versus the result of the actual, sterile and legal silicone product. Nonetheless, foreign body reactions and granulomas are possible with any injectable implant, temporary or permanent. Injectors need to be aware of this and employ appropriate treatment protocols.
Nasal deformities commonly treated with NSR
Correction of a mild to moderate dorsal hump is probably the most common type of NSR. The hump is not eliminated; it is merely camouflaged by dermal filler in the dorsum, superior and inferior to hump as needed. Often, filler is also placed in the radix to balance the increased volume to the dorsum with the added benefit of widening the naso-frontal angle (Figure 6). At times it is desirable to augment the radix to lengthen the appearance of a short or stubby nose (Figure 6).
A polly beak deformity is the over-projection of the cartilaginous nasal dorsum compared to the bony dorsum. It can be genetic or iatrogenic, the adverse sequelae of a surgical rhinoplasty30. This can be improved by columellar elevation and equalisation of the cartilage-bone transition with filler31. Columellar elevation and injection of the infradomal of the tip area can create the illusion of cephalic tip rotation9 and help balance the convexity of the polly beak deformity.

Figure 6 0.5 cc’s hyaluronic acid to disguise a dorsal hump and widen the nasofrontal angle.
(A) Before, (B) after
The opposite of a hump or a polly beak deformity, a saddle nose, can also be effectively treated with NSR. A saddle nose occurs when there is a concavity of the dorsum, instead of a straight slope or a convexity causing a hump. It is usually related to prior rhinoplasty, a collapse of septal support, septal perforation or trauma15. A straighter, smoother dorsum can be often accomplished with a small amount of filler at the trough of the dorsal dip. CaHa fillers may be best for this purpose because of their higher G’ and n*, allowing moulding of the product and prevention of lateral diffusion of the product. Injections are best performed in the midline, as there is less risk for intravascular injection.
Widening of the nasolabial angle has the effect of lifting the tip of the nose. Filler is injected at the anterior nasal spine and if needed, can also be placed at the columellar base8. Care should be taken not to widen this area too much. Lifting the tip helps the nose to appear more dainty and feminine. A masculine droopy tip can be lifted in a similar fashion with more attention to the columella and less filler to the nasal spine. Sometimes a ‘splint’ of filler between the length of the medial crura is needed to achieve lift in heavier male tips.
Patients with a wide or flat appearing nose due to a low dorsum are good candidates for NSR. These patients can also exhibit psuedotelecanthus, an optical illusion that makes the eyes appear too far apart15. Augmentation with filler in the midline of the dorsum can add projection, which will give the illusion of a narrower nose and may reduce the psuedotelecanthus effect15. Once again, a high G’ and n* product is best for this purpose.
A crooked or twisted appearing nose can be treated, to a certain extent, with NSR. Filler placed on the lateral nasal wall exhibiting the concavity will balance the opposite convexity to a certain degree. In some cases, there is a concavity or convexity without an opposite response on the other side. These distortions are relatively straightforward to fix. A sidewall concavity is easily filled, as long as intravascular injection is avoided. A sidewall convexity, like a dorsal hump, can be treated by injecting filler cephalad and caudal to the convexity to minimise its size and then balanced on the opposite side. During this treatment, it is easy to add too much volume and wind up with a large, wide, and over-projected nose. Patient selection is therefore probably the factor that contributes most to the success or failure of this particular application.
Cartilaginous defects, either genetic or iatrogenic can be reduced with an injectable filler. The nasal tip is an area where good results can be obtained with small volumes of filler, but it is also an area where a risk of vascular compromise to the skin envelope is increased9. A bifid tip, retracted or under rotated tip, retracted/notched alar cartilages, asymmetric tip defining points all can be smoothed and/or camouflaged with minimal product and minimal downtime for the patient. This is often a rewarding area to treat as the patient can see instant improvement after a short, relatively pain-free appointment.
Complications of NSR
The greatest concern when treating the nose is the intra-arterial injection of the product32. The literature has well-documented cases of brain infarction, skin necrosis and blindness from injecting fat, fillers and volumizers32,33 intra-arterially. While injection to any facial site can cause arterial compromise, researchers in Singapore reported that injections into the nose and glabella form the vast majority of reported cases of blindness34. It is important to recognise and promptly treat this devastating complication.
 Blindness resulting from filler embolisation in the eye occurs within seconds after injection, regardless of ocular pain in the affected eye34. Ophthalmic artery occlusion is characterised by severe ocular pain, minutes after injection. On the other hand, central retinal and branch artery occlusion may present with vision loss but without ocular pain34. Sudden onset of non-ocular facial pain or headache with loss of vision or visual field defect is possible as well35. Other ocular signs such as deviation of the globes, pupillary defect, horizontal strabismus, ptosis and corneal oedema34, 35 are possible.
Blindness resulting from filler embolisation in the eye occurs within seconds after injection, regardless of ocular pain in the affected eye34. Ophthalmic artery occlusion is characterised by severe ocular pain, minutes after injection. On the other hand, central retinal and branch artery occlusion may present with vision loss but without ocular pain34. Sudden onset of non-ocular facial pain or headache with loss of vision or visual field defect is possible as well35. Other ocular signs such as deviation of the globes, pupillary defect, horizontal strabismus, ptosis and corneal oedema34, 35 are possible.
If retinal or ophthalmic artery embolism is suspected, the patient must be transferred at once to the nearest eye specialist via ambulance. No safe, feasible, and reliable treatment exists for iatrogenic retinal embolism36. However, while awaiting the ambulance, the non-ophthalmologist injector can take action to try to re-perfuse the retina. These include flooding the treated area with hyaluronidase, ocular massage to try to dislodge the emboli and attempting rapid changes in intra-ocular pressure to try to dislodge the emboli (applying pressure to the sclera and releasing every few seconds)35. Other treatments are aimed at increasing blood flow and O2 delivery and decreasing IOP36. These include supplemental oxygen, nitro paste, timolol eye drops and acetazolamide IV or PO34.
A cerebral infarct is a rare complication and occurs by much the same route as a retinal infarct. There are numerous case reports in the literature detailing cerebral infarct after various types of filler injected to the nose, peri-nasal area, and glabella37–40. Symptoms can include the aforementioned ocular issues, headache, paraesthesias, weakness, aphasia37,38 as well as paralysis39,40. This is a medical emergency and the patient must be transferred to a tertiary care centre post-haste.
Skin necrosis is another possible sequelae of intra-arterial injection or even compression. Immediate symptoms include severe pain and blanching or pale appearance15, which can be hard to distinguish from blanching secondary to epinephrine containing anaesthetics. Within hours a livedo reticularis appearance of mottled blue to purplish discolouration can appear. Within a few days, blisters can appear41. If unilateral, it can appear to be a herpetic outbreak but will not respond to antivirals or steroids. Typically, the vesicles associated with herpetic eruption are filled with clear fluid, whereas pustules may be more indicative of necrosis9.
The more mundane filler complications can occur with NSR and must not be discounted. Bumps and nodules, granulomas and biofilms, Tyndall effect, inflammation, infection, and hematomas are all possibilities that the injector must be prepared to diagnose and treat. These complications are not unique to NSR and have various treatment protocols.
Conclusion
In the right patient, NSR can be a remarkably effective and quick treatment with a high satisfaction rate. Injectors must be knowledgeable of nasal anatomy and the best methods for camouflaging irregularities or creating the optical illusion of a smaller, straighter nose. Knowledge of the rheological and hydrophilic properties of the various fillers available and which to use for each application in NSR is essential. Avoidance of danger zones and attention to technique will help minimise complications. Injectors need to be aware of the possible devastating complications from NSR and have a treatment plan in place. Despite its risks, NSR may be less risky than a traditional rhinoplasty. As a rule, the patient and physician must decide together the best plan for that patient, whether it is no treatment, NSR or surgical rhinoplasty.
Declaration of interest None
Figures 1-6 © Amy Miller
References:
- Hunter B, Mullan G. Non-surgical Rhinoplasty. Aesthetics Journal. 2016 available at https://aestheticsjournal.com/feature/non-surgical-rhinoplasty [Last accessed August, 2018]
- Adamson PA, Warner J, Becker D, Romo TJ, Toriumi DM. Revision Rhinoplasy: panel discussion, controversies and techniques. Facial Plast Surg Clin North Am. 2014;22(1):57-96.
- Kontis TC, Lacombe VG. Cosmetic Injection Techniques: A Text and Video Guide to Neurotoxins and Fillers. Thieme Medical Publishers, Inc. NY. 2013.
- Coimbra DD, deOliveira BS, Uribe NC. Nasal filling with a new hyaluronic acid: a series of 280 cases. Surg Cosmet Dermatol 2015;7(4):320-6.
- Bravo BSF, Bravo LG, Da Rocha M, et al. Evaluation and Proportion in Nasal Filling with Hyaluronic Acid. J Clin Aesthet Dermatol. 2018;11(4):36-40.
- Redaelli A, Limaro P. Minimally Invasive Procedures for Nasal Aesthetics. J Cutan Aesthet Surg. 2012;5(2):115-20.
- Naini FB, Cobourne MT, Garagiola U, et al. Nasofrontal Angle and Nasal Dorsal Aesthetics: A Quantitative Investigation of Idealized and Normative Values. Facial Plast Surg. 2016;32(4):444-51.
- De Maio M, Rzany B. Injectable Fillers in Aesthetic Medicine. Springer, 2014.
- Jasin, ME. Non surgical Rhinoplasty Using Dermal Fillers. Facial Plast Surg Clin N AM. 2013;21:241-52.
- Toriumi DM, Mueller RA, Grosch T, et al. Vascular anatomy of the nose in the external rhinoplasty approach. Arch Otolaryngol Head Neck Surg. 1996;122:22-34.
- Kim SK, Kim JC, Lee KC et al. Correction of the Supratip Deformity of the Nose. Aesthetic Surg J. 2012;32(8):943-55.
- Balasubramanian T. Local Anesthesia of the Nose and Nasal Cavitiy-A Review. Glob J Oto. 20174(4): 555643.DOI: 10.19080/GJO.2017.04.55564
- Molliex S, Navez M, Baylot, J et al. Regional Anaesthesia for outpatient nasal surgery. British Journal of Anaesthesia. 1995;76:151-53.
- Kurkjian TJ, Ahmad J, Rohrich RJ. Soft-Tissue Fillers in Rhinoplasty. Plast and Reconstr Sur. 2013;133:121e-26e.
- Johnson ON, Kontis TC. Nonsurgical Rhinoplasty. Facial Plast Surg. 2016;32:500-6.
- Wang LL, Friedman O. Update on injectables in the nose. Curr Opin Otolaryngol Head Neck Surg. 2017;25:307-13.
- Kim B. The Basics of Dermal Filler. Investigative dermatology and Venereology Research. 2015. Available at: www.ommegaonline.org/article-details/Basics-of-Dermal-Fillers/628 [last accessed Sept, 2018] https://doi.org/10.15436/2381-0858.15.628
- Sundaram H, Voigts B, Beer K, et al. Comparison of the rheological properties of viscosity and elasticity in two categories of soft tissue fillers: calcium hydroxyapatite and hyaluronic acid. Dermatol Surg. 2010;36:1859-65.
- Bowman PH, Narin RS. (2005) ‘Hylans and Soft Tissue Augmentation Soft Tissue Augmentation’,In: Carruthers J and Carruthers a. Eds. Soft Tissue Augmentation, Philadephia, PA Elsiever 1st ed. 33-53.
- Micheels M, Eng MO. Rheological Properties of Several Hyaluronic Acid-Based Gels: A Comparative Study. J Drug Dermatol. 2018;17(9):948-54.
- Humphrey CD, Arkins JP, Dayan SH. Soft Tissue Fillers in the Nose. Aesthet Surg J. 2009;29(6):477-484.
- Thomas WW, Bucky L, Friedman O. Injectable in the Nose: Facts and Controversies. Facial Plast Surg Clin N Am. 2016;24:379-89.
- Lin S, Hsiao YC, Huang JJ, et al. Minimal Invasive Rhinoplasty: Fat Injection for Nasal Dorsum Contouring. Annals of Plastic Surgery. 2017;78:s117-23.
- Kao WP, Lin YN, Lin TY. Microautologous Fat Transplantation for Primary Augmentation Rhinoplasty: Long-Term Monitoring of 198 Asian Patients. Aesthetic Surgery Journal. 2016;36(6):648-56.
- Montral J. Fat Grafting to the Nose: Personal Experience with 36 Patients. Aesthetic Plast Surg. 2011;35(5):916-22.
- Rivkin A. A Prospective Study of Non-Surgical Primary Rhinoplasty Using a Polymethylmethacrylate Injectable Implant. Dermatol Surg. 2014;40:305-313.
- Chen L, Li SR, Yu P, et al. Comparison of Artecoll, Restylane and silicone for augmentation rhinoplasty in 378 Chinese patients. Clin Invest Med. 2014;37(4):E203-10.
- Webster RC, Hamdan US, Gaunt JM, ET AL. Rhinoplastic revisions with injectable silicone. Arch Otolaryngol Head neck Surg. 1986;112(3):269-76.
- Park ME, Curreri AT, Taylor GA, et al. Silicone Granulomas, a Growing Problem? Jour Clin Aesthet Dermatol. 2016;9(5):48-51.
- Bray D, Hopkins C, Roberts DN. Injection rhinoplasty: non-surgical nasal augmentation and correction of post-rhinoplasty contour asymmetries with hyaluronic acid: how we do it. Clinical Otolaryngology. 2010;35:220-37.
- Schuster B. Injection Rhinoplasty with Hyaluronic Acid and Calcium Hydroxyapatite: A Retrospective Survey Investigating Outcome and Complication Rates. Facial Plast Surg. 2015;31:301-7.
- Hunter B, Mullan G. Non-surgical Rhinoplasty Part 2. Aesthetics Journal. 2016 available at: https://aestheticsjournal.com/feature/non-surgical rhinoplasty-part-2-1 [last accessed Aug. 2018]
- DeLorenzi C. Complications of Injectable Fillers, part 1. Aesthet Surg J. 2013;33:561-75.
- Loh KTD, Chua JJ, Lee HM, et al. Prevention and Management of Vision Loss Relating to Facial Filler Injections. Singapore Med J. 2016;57(8):438-443.
- Townshend, A. Blindness After Facial Injection. J of Clin Aesthet Derm. 2016;9(12):e5-7.
- LazzeriD, Agostini T, Figus M, et al. Blindness following cosmetic injections of the face. Plast Reconstr Surg. 2012;129(4):995-1012.
- Li KT, Huang YH, Chen CH, et al. Delayed onset cerebral infarction after cosmetic facial injection using hyaluronic acid. J Formosan Medical Association. 2016;115:587-588.
- Yoon SS, Chang D, Chung KC. Acute fatal stroke immediately following autologous fat injection into the face. Neurology. 2003:61(8):1151-2.
- Kim EG, Eom TK, Kang SJ. Severe visual loss and cerebral infarction after injection of hyaluronic acid gel. J Craniofac Surg. 2014;25(2):684-6.
- Lee S, Jung JH, Seo J, et al. Ischemic Stroke Caused by a Hyaluronic Acid Gel Embolism Treated with Tissue Plasminogen Activator. J Neurocritical Care.2017;10(2):132-135.
- Manafi A, Barikbin B, Manafi A, et al. Nasal Alar Necrosis Following Hyaluronic Acid Injection into Nasolabial Folds: A Case Report. World J Plast Surg. 2015;4(1):74-8






{kind=link}