

Norbert Kang outlines his treatment approach for prominent ears using the Earfold® implant, which can be used in
patients aged 7 years and over
An ear which projects by more than 20 mm from the side of the head is often perceived as prominent by other observers1. By this estimate, up to 2% of the worldwide population are affected by prominent ears* 2,3 and up to half of the adult population with prominent ears are likely to be concerned about them* 4. Both ears
are commonly affected although in 10% of cases, just one side
is prominent.
Prominent ears are a concern because of the negative psychological impact that they may have on the psyche2. This is a particular problem in childhood when prominent ears may draw unwanted attention and comments from other children and can result in significant bullying and teasing2. Patients often tell me of hurtful comparisons being made to ‘Dumbo’, ‘FA-cup’ or ‘wing-nut’. Sadly, the dislike of prominent ears seems to be universal with most cultures on the planet using similar pejorative terms to describe prominent ears (e.g. ‘sail-ear’ in Germany). This can lead to significant changes in the behaviour of the children5 who then avoid all activities or situations in which their ears are exposed or visible (e.g. sports). These behaviours and concerns often linger on into adulthood — if correction is not performed. Fortunately, the evidence for major improvement in self-esteem after surgical correction of the prominence is irrefutable5,6.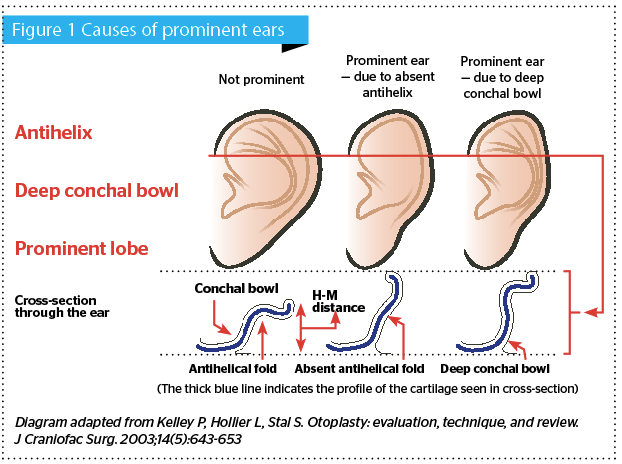
Ears are prominent either because of a poorly formed or absent antihelical fold7–9 (Figure 1) or because of a deep conchal fossa7 (Figure 1). Both of these abnormalities may need to be addressed when correcting prominence of the ear. However, before the introduction of the Earfold® (Allergan, Marlow, UK) implant, the only way to correct either of these problems was to undertake standard otoplasty. Otoplasty refers to any procedure to reshape the ear — either surgical or non-surgical. Treatment of prominent ears with Earfold is a form of surgical otoplasty, which is minimally invasive.
Existing treatment options for prominent ears
Standard otoplasty surgery comes in various forms but most surgeons who carry out otoplasty will routinely use a combination of surgical steps that involve the use of sutures and/or cartilage sculpting. This is highly complex and invasive surgery8, which typically takes 45–60 minutes per ear10,11 and is, therefore, best performed by surgeons who are experienced in the techniques used to limit the risk of complications or poor outcomes. In the hands of an expert, the results are usually durable and reproducible. However, the learning curve to become an expert is steep and long. Even in the hands of an expert, problems such as asymmetry and recurrence of prominence can occur10.
 To avoid the problems inherent with surgical otoplasty surgery — namely the time needed to learn the surgical technique, the time needed to perform the surgery, and the complications which can ensue8, a number of non-surgical otoplasty techniques have been used;
To avoid the problems inherent with surgical otoplasty surgery — namely the time needed to learn the surgical technique, the time needed to perform the surgery, and the complications which can ensue8, a number of non-surgical otoplasty techniques have been used;
- Earbuddies™ 12
- Sorribes (previously known as Auri®Method)13.
These two techniques rely on the fact that typically up to the age of 5 years, human ear cartilage can be remodelled by application of an external force. Therefore, they use a variety of splints or plasters that can be applied to the outside of the ear to deform the cartilage over a prolonged period of time (between 2 weeks and 6 months). The cartilage responds to the force applied by the external splints and changes its shape accordingly, thereby correcting the prominence of the ear. However, in order to be completely effective, the splints must be worn correctly and continuously. Partial compliance with treatment results in only partial correction. As a result, patients may experience no correction, partial correction, and/or continuing asymmetry. Over a certain age (which varies from one individual to another), the cartilage becomes increasingly thick and stiff and unresponsive to external splintage. When this happens, surgical otoplasty in some form becomes necessary.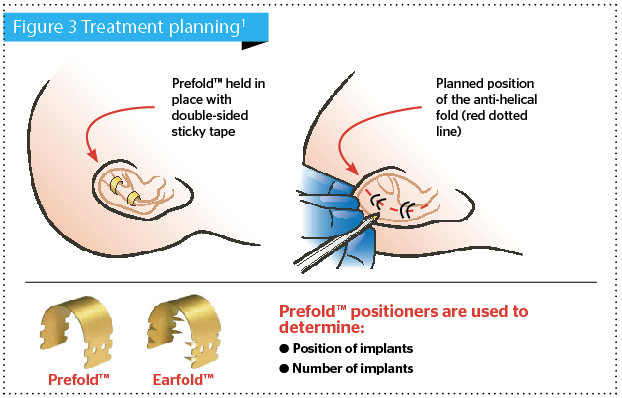
Introduction to Earfold®
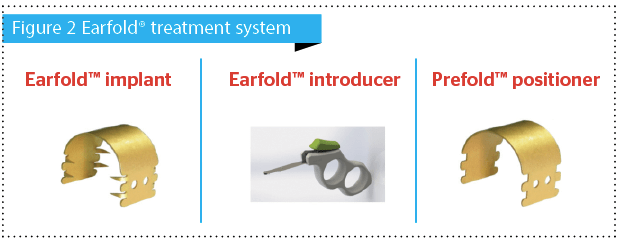
To avoid some of the problems inherent in standard surgical and non-surgical otoplasty techniques9, I devised a new approach to treatment that uses a small, permanent, metal implant called Earfold®. The implant is made of a thin strip of metal alloy (nickel and titanium) which is coated with a thin layer of 24-carat gold (Figure 2)11. The alloy has a number of important properties including super-elasticity and shape memory. Therefore, when inserted into the front of the ear, Earfold® is able to fold and reshape the underlying cartilage according to the shape that has been pre-programmed into the implant1,11.
My intention was to offer patients and surgeons a treatment option that:
- Was more predictable, which is particularly important in cases of asymmetry1,11
- Offered patients some degree of control over the final outcome since they can view the likely result before the procedure1,11
- Had lower rates of recurrence — with the implant in place1,11
- Was reversible and correctable — if the implant is removed1,11
- Has low infection rates (typically 1.6%) — easily treatable with oral antibiotics1,11
- Has low implant exposure rates (3–4%), which are easily dealt with by removal1,11
- Is quick (15–20 minutes to insert four implants), which makes it possible to perform the treatment under local anaesthesia, even in children. The lower age limit is seven years. There is no upper age limit1
- Can be used to salvage cases of residual prominence, e.g. after suture-based standard otoplasty1,11.
The Earfold® implant is designed to create or enhance the shape of the antihelical fold of the ear (Figure 1). Therefore, it is not suitable for use in every patient with prominent ears and pre-operative, patient selection is critical to success. That said, Earfold® can still have a beneficial effect in selected patients with prominence due to a deep conchal bowl (Figure 1)1,11 where the implant can be used to roll the lateral wall of the concha into the reformed antihelical fold.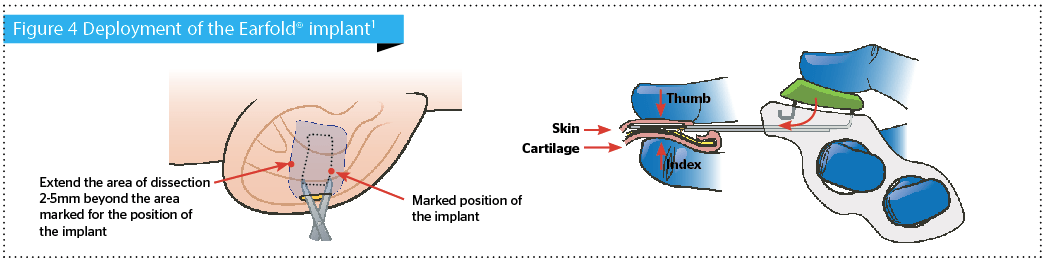
How Earfold treatments are performed
Treatment with Earfold® begins with a careful pre-operative assessment using Prefold® positioners (Figure 2 and 3). I ask my patients to sit in front of a mirror and ask them to show me how they would like their ears to look1,11. This gives me a good early indication of whether or not Earfold® will work for them. If the majority of the correction they are looking for requires an enhancement in the shape of their antihelix, then that is a good indication that Earfold® will be appropriate for them. If not, then it may be necessary to use an alternative surgical approach.
To do this, I show the patients the sort of correction they can achieve with Earfold® by using Prefold® positioners (Figure 3)1. Prefold® is identical in shape, size and elasticity to the Earfold® implant but without the sharp metal tines that are needed to grip the cartilage when Earfold® is released into the ear. Therefore, Prefold® can be used to predict where each Earfold® implant must be placed to reshape the antihelical fold to correct the prominence perceived by the patient1,11. It is this predictive ability that makes the Earfold® treatment system so powerful and is one of the many unique attributes of this approach1,11. Prefold® takes away much of the guesswork involved in standard surgical otoplasty and gives the patient some measure of control over the (likely) outcome1,11.
 Once a decision has been made on the position and number of implants required by the patient, surgery to insert the implant can be performed. This is usually performed under local anaesthetic, although in children, a short general anaesthetic could be used11. The position of each implant in relation to the planned position for the new, or enhanced, antihelical fold is carefully marked on the anterior skin of the ear (Figure 4)1. The local anaesthetic allows the surgeon to hydro-dissect the soft-tissues of the anterior surface of the ear. An incision (8mm long) is made at a minimum of 2–3 mm away from the proximal edge of the future footprint of the implant. A subcutaneous/subperichondrial pocket is created to allow the implant to be inserted using a special introducer (Figure 4). The implant is then released onto the anterior surface of the cartilage reshaping it immediately and thereby correcting the prominence of the ear. A single suture is used to close the incision and the wound is then dressed with a single Steri-Strip®. No other dressings are necessary.
Once a decision has been made on the position and number of implants required by the patient, surgery to insert the implant can be performed. This is usually performed under local anaesthetic, although in children, a short general anaesthetic could be used11. The position of each implant in relation to the planned position for the new, or enhanced, antihelical fold is carefully marked on the anterior skin of the ear (Figure 4)1. The local anaesthetic allows the surgeon to hydro-dissect the soft-tissues of the anterior surface of the ear. An incision (8mm long) is made at a minimum of 2–3 mm away from the proximal edge of the future footprint of the implant. A subcutaneous/subperichondrial pocket is created to allow the implant to be inserted using a special introducer (Figure 4). The implant is then released onto the anterior surface of the cartilage reshaping it immediately and thereby correcting the prominence of the ear. A single suture is used to close the incision and the wound is then dressed with a single Steri-Strip®. No other dressings are necessary.
At this point, I usually sit my patients up to allow them to see the correction achieved in a mirror. If any final adjustments are needed, these can be done immediately (e.g. repositioning an implant). Patients are often surprised at how different they look immediately after the implants have been inserted but I warn them that this will change temporarily within the next 24–48 hours, as soft-tissue swelling develops. Most of the swelling will have gone by the end of the first week, especially if their treatment involves use of Earfold® implants only.
 I advise all my patients to avoid sleeping on their sides/ears for 3–4 weeks and to avoid swimming and contact sports for a similar period. They may also wish to use a Velcro® secured, removable headband at night, for 6–8 weeks. These measures1 will help to avoid the possibility of flexing their ears before the implants have settled in, since movements of the ear after surgery can result in the implant becoming dislodged. If this were to happen, the implant could become visible and the suboptimal position of the implant might also interfere with the correction of the prominence.
I advise all my patients to avoid sleeping on their sides/ears for 3–4 weeks and to avoid swimming and contact sports for a similar period. They may also wish to use a Velcro® secured, removable headband at night, for 6–8 weeks. These measures1 will help to avoid the possibility of flexing their ears before the implants have settled in, since movements of the ear after surgery can result in the implant becoming dislodged. If this were to happen, the implant could become visible and the suboptimal position of the implant might also interfere with the correction of the prominence.
Although patients will feel no pain for the first 4–5 hours after treatment, some discomfort is inevitable once the local anaesthetic has worn off and typically lasts for 2–3 days in most cases. Most of the post-operative swelling and bruising will resolve in the first 1–2 weeks after treatment, however, some patients may also experience some degree of sensitivity for up to 3 months (e.g. when holding a telephone against the ear) — but that depends on the patient1,11.
Conclusion
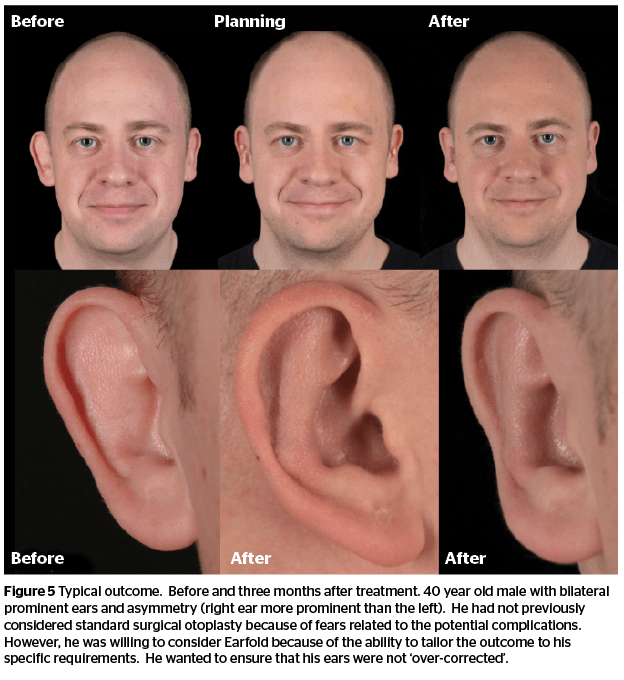
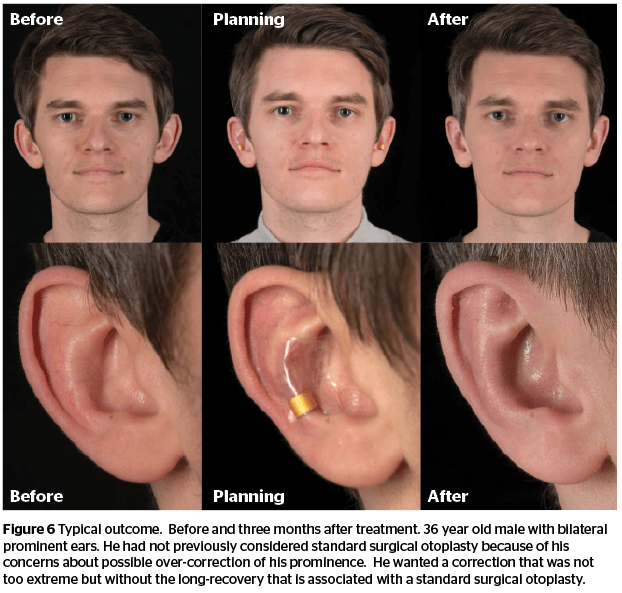
Earfold® has now been in use since 2011. The data we have so far11 confirms that treatment with the implant produces durable and consistent correction of prominent ears with low rates of infection and relatively low rates of implant extrusion. When complications do arise, they are simple to correct. Experience has shown that treatment is reversible if the implants are removed within the first few months after treatment. With the passage of time (years), the cartilage does remodel (especially in children) so the effects become increasingly permanent even if the implant is removed. However, patients are advised to leave the implants in place permanently in order to get the best effects. Further studies are ongoing to examine patient satisfaction and aesthetic outcomes in detail.

