


Nail psoriasis
Nail psoriasis is common and observed in approximately 50% of all psoriatics; however, the life-long risk to develop nail changes is estimated at 90% 35. Psoriatic nail alterations are notoriously difficult to treat, although they are said to respond to systemic treatment when this is successful.
Three studies of laser treatment have been published. In the first, 61 nails were treated with photodynamic therapy (PDT) and 60 nails treated with a pulsed dye laser (PDL), pulse duration 6 ms, 9 J/cm2. A decrease in the nail psoriasis severity index (NAPSI) score was observed with both treatments and in both nail matrix and nail bed involvement. No statistical differences were observed between PDT and PDL (at baseline P = 0.632; at 3 months P = 0.084; and at 6 months P = 0.535), and between nail matrix and nail bed NAPSI scores (P = 0.423 and P = 0.853, respectively) 36. The second trial used 595 nm PDL once per month for 3 months. Pulse duration was 1.5 ms, laser energy 8–10 J/cm2, beam diameter was 7 mm 37. Despite the considerably shorter pulses, there was a statistically significant improvement of the NAPSI scores, particularly with regard to onycholysis and subungual hyperkeratosis.
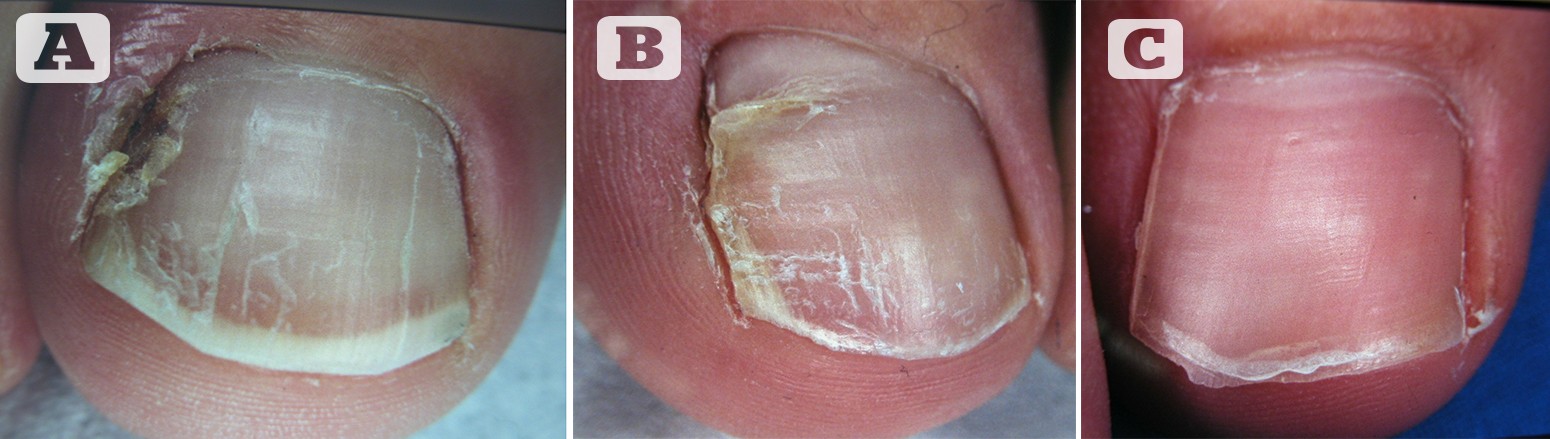
Figure 2 Before and after surgery for ingrown toenail. (A) Ingrown hallux nail before surgery (B) 3 months after surgery (C) The toe 1 year after surgery
The most recent study compared long and short pulse PDL treatment. The results were obtained with variable pulse durations and fluences — 6 ms pulses with 9 J/cm2 in 40 nails and 0.45 ms pulse duration with 6 J/cm2 in 39 nails were virtually identical; the only difference was statistically significant lower pain levels in the shorter pulse group38. Therefore, the concept that angiogenesis is a major factor in the activity of psoriatic lesions appears to be supported by coagulating blood vessels with the dye laser.
Subungual haematomas and various tumour-like lesions
Subungual haematoma is a painful sequela of an acute trauma and decompression is the immediate treatment of choice if a serious bone fracture has been ruled out. Drilling a hole into the nail is a generally accepted treatment; however, this can also easily be done without pain using a CO2 or Er: YAG laser 39.
Ungual tumours often pose therapeutic problems. Laser treatments with a lower risk of permanent postoperative nail dystrophy appear to be tempting.
A subungual haemangioma was successfully treated with a PDL using its selective action of haemoglobin 40. Pyogenic granuloma, which in fact is an eruptive angioma, can be treated effectively with a PDL 39. Granulation tissue from ingrown and pincer nails also promptly reacts to PDL 42, but can also be vapourised with a CO2 laser. Multiple periungual fibromas are easily removed with a CO2 laser with good cosmetic results 43.
Human papillomavirus induced warts are rapidly vapourised or carbonised with a CO2 laser 43–47 but can also be necrotised with a Nd: YAG laser, whereas the PDL aims at coagulating the blood-filled dilated capillaries in the papillae of the warts 48. Digital myxoid pseudocysts were vapourised with the CO2 laser, but one third recurred 49. Laser vapourisation was also used to remove peri and subungual Bowen’s disease.
Conclusions
Laser applications are now an integral part of the diagnosis and treatment of many systemic and dermatological disorders. Their use for nail conditions is increasing as this literature review has demonstrated. While it may be tempting to use lasers frequently in order to amortise them, alternative treatments may be available at a lower cost. The studies mentioned in this review — and future studies — will aid in the education of practitioners of how and when it is most appropriate to use lasers for the treatment of nail conditions.

