


Identifying the injection points
To illustrate the precise procedure, Figures 2–4 show the typical injection points for 3D volumisation.
Top half of the face
Figure 2 shows the entry point on the cheek bone curve. It is placed at the middle point between the top and bottom edges of the zygomatic bone.
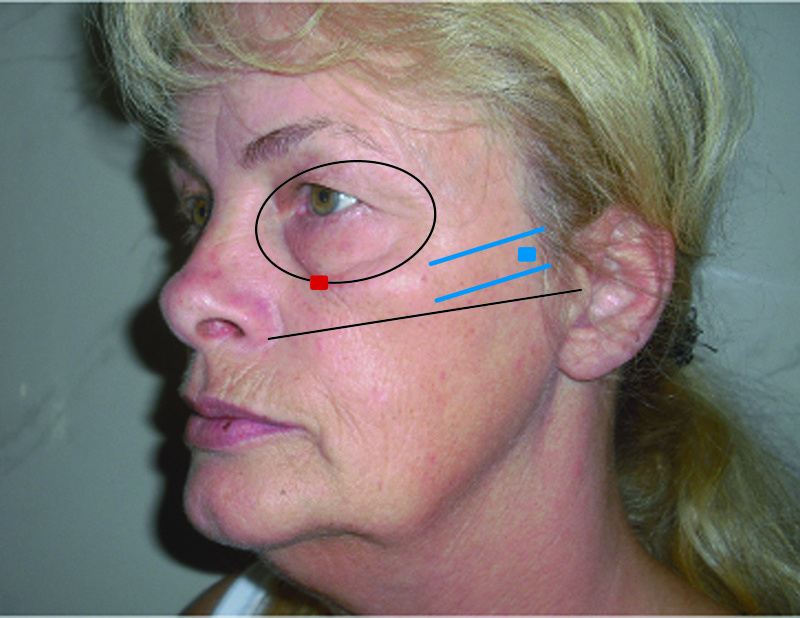
Figure 2 Cheek bone curve injection point
For the second point it is necessary to find the highest point of the cheek, or the ideally highest point (the point of maximum anterograde projection). A perpendicular line from the outer orbital margin has to projected vertically downwards. The second line goes from the middle of the chin upwards through the corner of the mouth. The intersection point of these two blue lines determines the point of the second injection (Figure 3).
Lower half of the face
Before an augmentation of the lower half of the face, a line should be drawn parallel to the tragus vertically downwards. At the point where this line meets the extension of the chin–jaw line, is the rearmost implantation point (near the angle of the jaw) from which the jaw line can be shaped (Figure 4).
Depending on the desired result, it may be necessary to place a number of entry points in the lower cheek area over the whole cheek area to place the filler in a fan shape in order to even out superficial wrinkles.
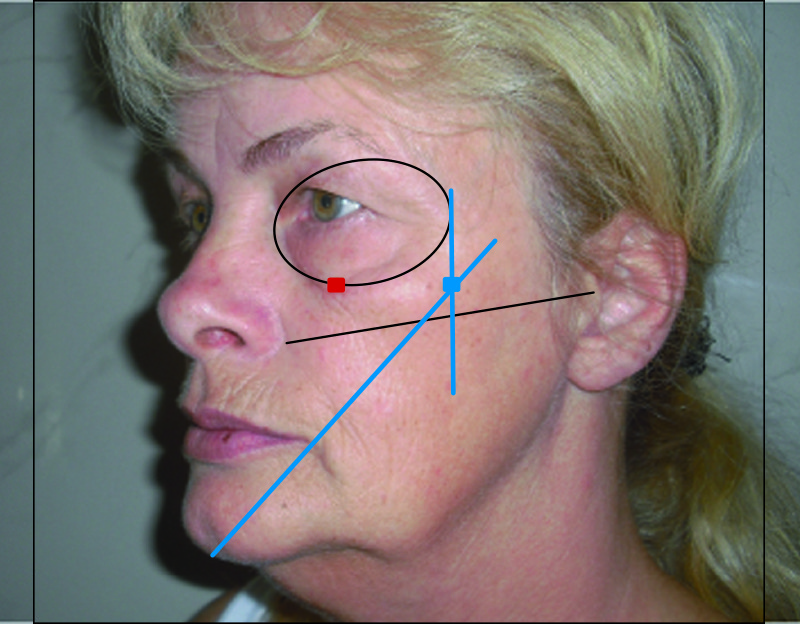
Figure 3 Central cheek injection point
Treatment and progress
The treatment begins with the first injection point on the cheek bone curve. A local anaesthetic may be administered to the entry point beforehand, after which a 1.5 cm-long, blunt-tip, flexible cannula is inserted in a medial ventral direction. Its tip comes to rest at the supraperiosteal area. A number of linear threads of CaHA should be placed in a fanning manner supraperiosteally. An even and sustained injection pressure is desirable. Correction should be completed to the clinical endpoint; overcorrection must be avoided. A typical fan is successfully carried out by using approximately 0.1 ml of material, but, of course, the amount will vary depending on the individual.
Using this injection technique, the treatment is continued in the same way from the second entry point (Figure 3). If an additional augmentation is required medially, another entry point is set; this usually runs perpendicular to the pupil. The third injection point can be seen in Figure 4. From this point a number of vectors can be placed in this direction towards the chin, thus reshaping the whole jaw line (CaHA to be placed supraperiosteally) and subdermally to treat the lateral cheek wrinkles in a crosshatch way (Figure 5 — showing the whole procedure). All treated areas are subsequently checked manually after implantation (moulding).
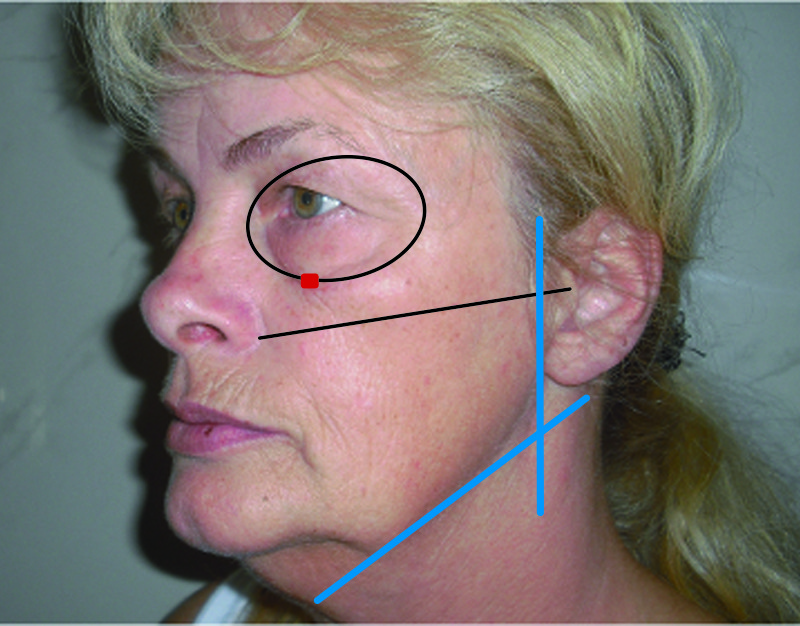
Figure 4 Jaw line injection point
Results
The immediately visible treatment results normally last 12 months or longer. Typical effects caused by the injections, such as reddening, low grade haematoma or swelling are in most cases unobtrusive and temporary. Touch-up treatments are seldom necessary.
This treatment methodology is the author’s personal approach, which has been developed over a number of years and from the author’s own experience. It is adaptable to many different facial features, and while there is more than one ‘recipe’ for treatment, it is necessary to provide some guidelines for treatment, as well as to define facial landmarks and entry points in order to successfully carry out this 3D vectoring treatment.

Figure 5 Mid-face 3D vectoring
Conclusions
The 3D vectoring technique represents a modern injection method for mid-face augmentation and lifting. The Radiesse volume filler with its high level of viscosity and elasticity, and consequently precise lifting capacity, is particularly suitable for this therapy. As a result of a technically perfect mid-face augmentation treatment, results can be achieved that show a particularly beautiful 3-dimensional reshaping and re-contouring.

