


Tretinoin
Tretinoin (retinoic acid) is the most commonly used topical retinoid for the treatment of melasma. It acts by removing melanin via keratinocyte shedding, enhances the penetration, and prevents the oxidation of HQ. It also reduces the risk of skin atrophy associated with the application of a topical corticosteroid as part of a combination bleaching formula31. Tretinoin is recommended at a concentration of 0.01–0.1%, and better results are obtained when it is used in a combination formula with HQ31,32. In a randomised study of 38 women with melasma, receiving topical tretinoin 0.1% for 40 weeks compared with placebo, resulted in improvement in 68% of patients compared to 5% of those using placebo33. However, tretinoin may result in erythema and scaling. During the treatment with tretinoin, sun exposure should be avoided and sunscreen applied sufficiently.
Combination formulae
The bleaching effect of HQ may be enhanced with a combination of other agents such as topical retinoids or topical corticosteroids. Combination therapy aims to increase efficacy, minimise side-effects, and shorten the duration of treatment. Combination formulae may contain two or three bleaching agents. The triple combination formula of HQ/retinoid/corticosteroid leads to better results, as the three ingredients act in combination and are better tolerated34. The best‑known triple combination formula of HQ/tretinoin/topical corticosteroid is the Kligman–Willis formula35. Application for 5–7 weeks is recommended. However, two drawbacks of this therapy is the use of high-concentration tretinoin (0.1%) and the use of a high-potency, fluorinated topical corticosteroid (dexamethasone)35.
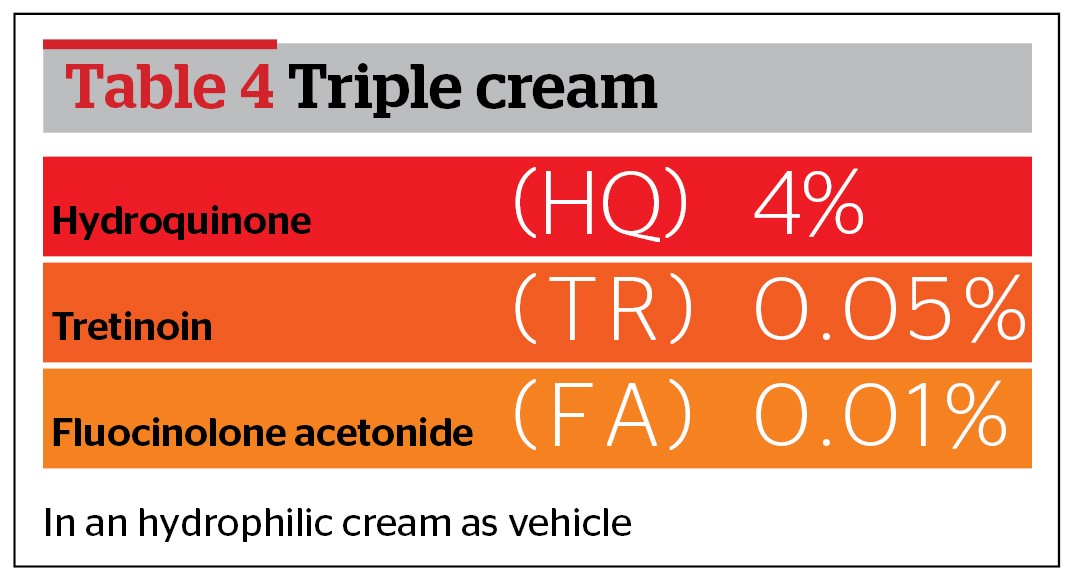
A modification using lower concentration of tretinoin (0.025–0.05%) and hydrocortisone as a topical corticosteroid has been proposed (Table 3)36. A further modification is the use of fluocinolone acetonide as a low-potency topical corticosteroid (Table 4). This modified formula resulted in complete clearance of melasma in 26% of patients, and a 75% reduction of melasma in 70% of patients34. This treatment is the first triple topical treatment that has been approved by the US Food and Drug Administration (FDA) for melasma34,38. Melasma has been associated with causing frustration, embarrassment and a negative influence on interpersonal relationships, but triple cream therapy may improve the quality of life of patients with melasma39.
Also, HQ may be used as a combination treatment either with a topical retinoid or glycolic acid (5–10%). Glycolic acid is an alpha hydroxy-acid (AHA) that reduces hyperpigmentation by the thinning of the stratum corneum and increased epidermolysis38.
Chemical peels, dermabrasion, lasers and light sources
Chemical peels remove excess melanin and superficial peels may be used for melasma in fair-skinned patients. On the other hand, peels should not be used for darker skin types as they are associated with a risk of post‑inflammatory hyperpigmentation (PIH) and aggravation of melasma40. Maintenance therapy with HQ 2% is recommended by the authors.
Dermabrasion is not traditionally used for melasma as it has been associated with side-effects such as PIH41.
Fractional laser therapy is the only laser treatment for melasma that has been approved by the US FDA, and it could be used as a third-line treatment in severe cases for patients who have not responded to other treatments and who are willing to accept the risk of post-procedure hyperpigmentation.42
Intense pulsed light (IPL), a non-laser light source that emits light with wavelengths between 515 and 1200 nm, has been reported to improve epidermal melasma by 76–100%41,43. It has therefore been proposed as an adjunctive therapy in combination with bleaching agents for better response and increased patient adherence to treatment41,43.
Evidence-based results and personal experience for treating melasma
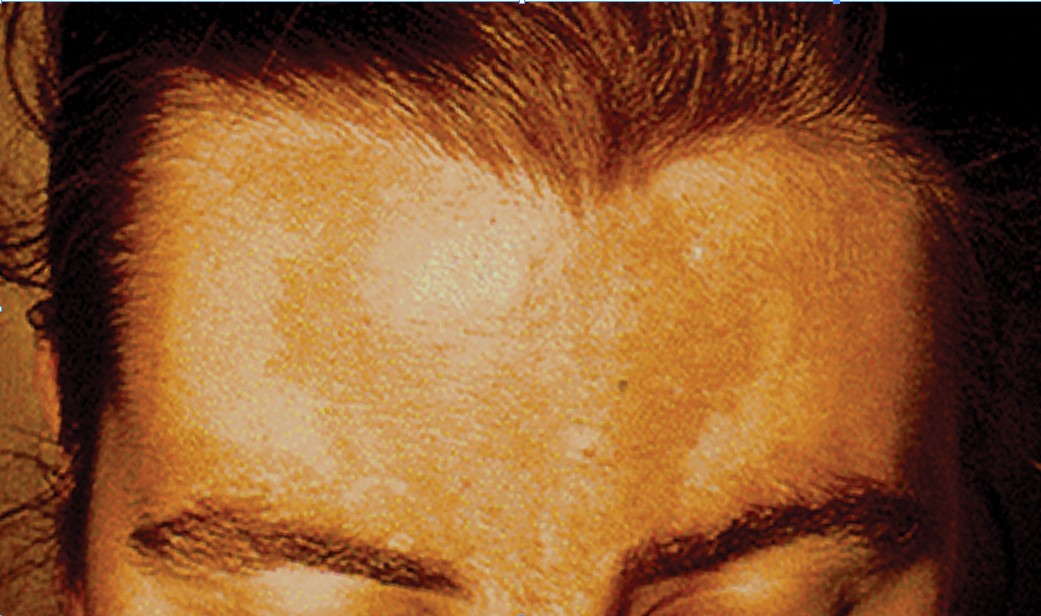
Figure 2 Melasma on the forehead
A recently-published systematic review of interventions used for the management of melasma identified only 20 eligible randomised controlled trials. All interventions, except tretinoin, were evaluated in one study each. It was reported that there is no standard therapy for melasma. Topical HQ (3–4%) was the most common topical monotherapy used. The triple-combination cream was more effective than any of the ingredients used in a dual‑combination cream in one study. No studies provided long-term data or quality of life results. The authors mentioned that the evidence was insufficient to provide guidance for the clinical practice of treating melasma owing to the poor methodology of the trials, the lack of standardised outcome measures, and the short duration of studies44.
Based on the lead author’s personal experience, the topical application of HQ 2–7% in combination with topical tretinoin (in concentrations up to 0.05%) is the preferred treatment for melasma. This combination may be used either in a combination formulae, applied once daily at bedtime, or by alternate application of HQ in the morning and tretinoin at bedtime. The daily application of sunscreen and the avoidance of sun exposure is necessary. In very resistant cases, fractional laser therapy may be proposed.
Conclusions
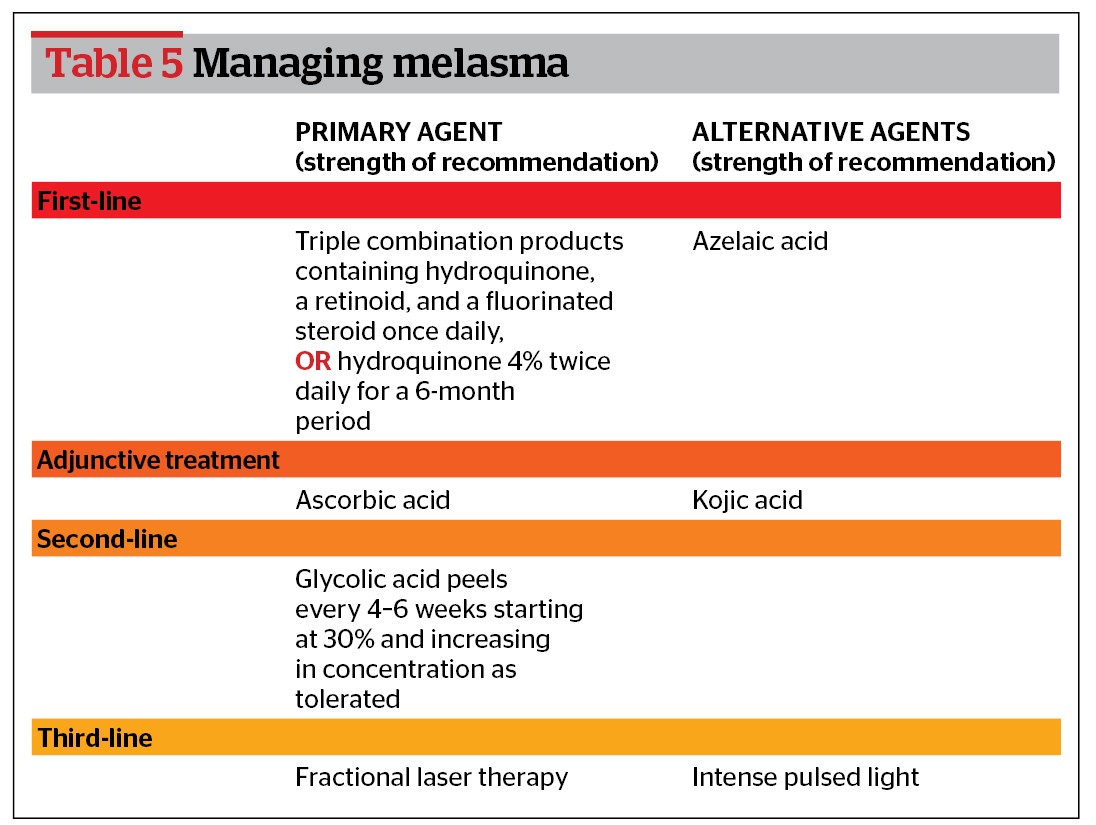
Melasma is a common, persistent pigmentation disorder that may profoundly affect the quality of life of patients. The therapeutic approach should encompass the avoidance of exacerbating factors, while combination treatments and maintenance therapy should be used for optimal results (Table 5)43, and treatment should be tailored to the individual patient.

