


Why just CO2?
In 2011, Balik et al investigated the effects of CO2 therapy with breathable air in an animal model. Results showed how the differences obtained in terms of lipolytic effect and the microcircular modifications were not statistically significant 15. Significant data has been obtained using different gases in experimental models, but they do not contraindicate the use of CO2 therapy.
However, Balik’s model had some bias. It was not built using a clearly described gas administration technique and protocol. Secondly, the researchers did not test the association between transcutaneous oxygen pressure (tcPO2 ) and laser Doppler flow because it is not easily applicable to the model used 16. Furthermore, the absence of toxicity of CO2 was not discussed and this is a key point to consider in the treatment of humans 16.
CO2 therapy devices
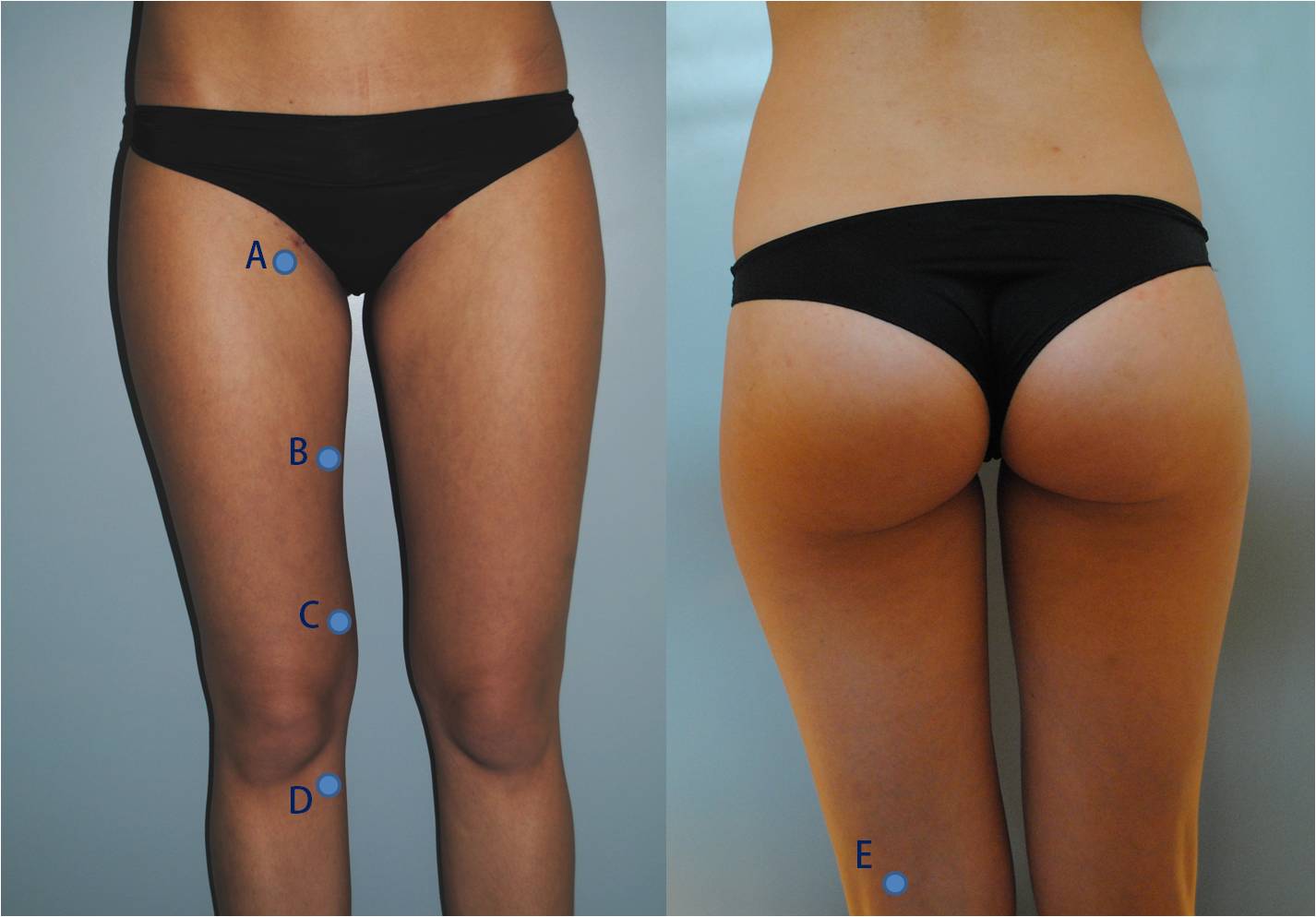
Figure 3 It is important to treat with small intradermal carbon dioxide infiltrations on landmarks along the great saphenous vein path. Point A = Crosse of great saphenous vein, point B = mid-thigh point, point C = Dodd’s perforator point, point D = Boyd’s perforator point, point E = popliteal fossa point
The safety and efficacy of this procedure strongly depend on the correct execution of the technique. For this reason, it is necessary to clarify the right characteristics of the devices:
-
Medical and sterile CO2 should be used
-
The equipment used should allow the physician to predetermine the purity of the gas administered; the quantity of gas to be infused; infusion time; the volume of gas administered; the temperature of the gas; the rate of infusion of the gas, which needs to be kept constant
-
The equipment must have certification to ensure it conforms with the technical data listed and the ability to be used for the administration of medical gas
-
A 30 or 32 gauge 13 mm needle should be used.
Treatment of cellulite and localised adiposities
The use of CO2 is related to its positive and documented effects on different aspects of the imperfection’s aetiology. Adipose tissue is a connective tissue composed of fat cells, stromal elements, blood and lymph vessels, and a matrix of collagen fibres. Clinical modification of connective tissue can be localised (adiposity) or diffuse (cellulite), and often coexist; for this reason they should be treated together.

Figure 4 Localised adipocity and early cellulite in a 28-year-old female patient (left). Results after eight treatments, anterior view (right)
Localised adipocity refers to the accumulation of fat in certain areas of the body (abdomen, thighs, trochanters, knees). The goal of therapy is to obtain a reduction in the volume of adipose masses; therefore, the use of CO2 is indicated either in combination with surgical treatments (in order to optimise and stabilise the results obtained) or alone, especially when patients refuse surgical treatments.
Cellulite refers to skin irregularities of the lower limbs related to sexual, genetic, and lifestyle factors, as well as incongruous clothing, such as high heels and tight pants. It can also be conditioned and aggravated by the presence of renal venous and/or lymphatic disease. It is a chronic condition and it is important to explain to patients how many times the treatment should be repeated, the manner and method of which, could differ in each case.
Treatment is based on a multidisciplinary approach, including lifestyle changes, the control of venous and/or lymphatic circulation, use of personalised diets, and medical and physiotherapy associated treatments, such as carbon dioxide therapy (used alone or in combination with other methods). Physiopathology of cellulite includes alterations to the microcirculation, venous, and lymphatic systems, which are influenced and worsened by the fat accumulation inside the connectival septa 8.
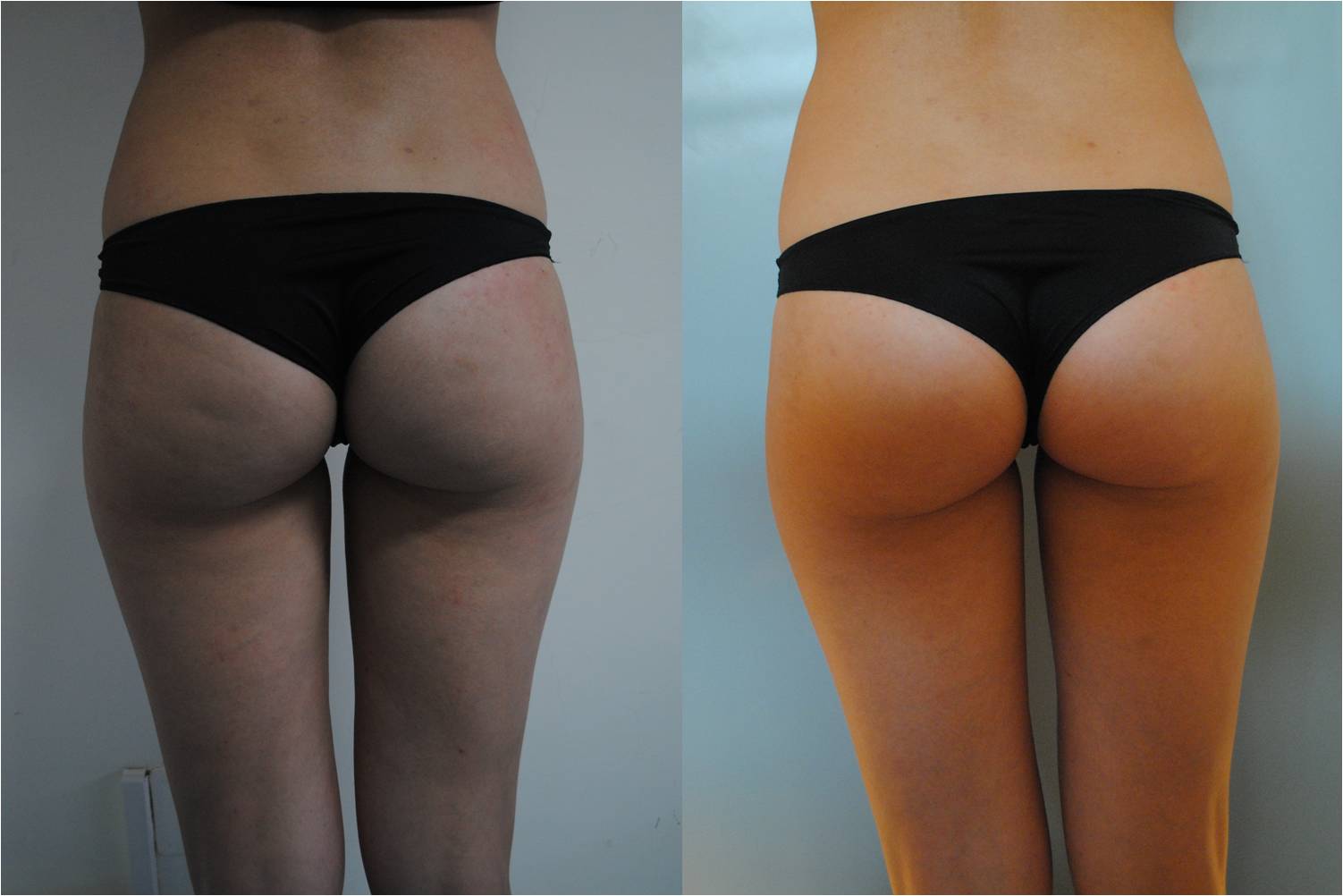
Figure 5 Localised adipocity and early cellulite in a 28-year-old female patient (left). Results after eight treatment, posterior view (right)
The administration of subcutaneous CO2 improves microcirculation by increasing blood flow in treated areas. This is achieved through the vasodilation induced by CO2 therapy, as well as changes in blood flow and vasomotion, which have been demonstrated by capillaroscopy, Doppler, and laser Doppler flow 6,7,8,12.
Furthermore, it has been shown that CO2 therapy increased oxygenation of peripheral tissues, owing to the artificial Bohr effect and the lipolytic action on adipose tissue, without damaging the connective tissue or reducing the adipose tissue thickness 8–10,16,17.
Figure 1 shows landmarks used to divide the different gluteal, trochanteric, and thigh regions. It is not necessary to infiltrate large volumes of CO2 to each area; rather, small amounts in the direction of the vectors shown in Figure 2 can be used. Furthermore, it is important to treat with small intradermal CO2 infiltrations along some key points on the great saphenous vein path. Figure 4 and Figure 5 show the reduction of the thigh’s circumference and skin quality in a young patient at the end of a complete treatment.
Treatment of stretch marks
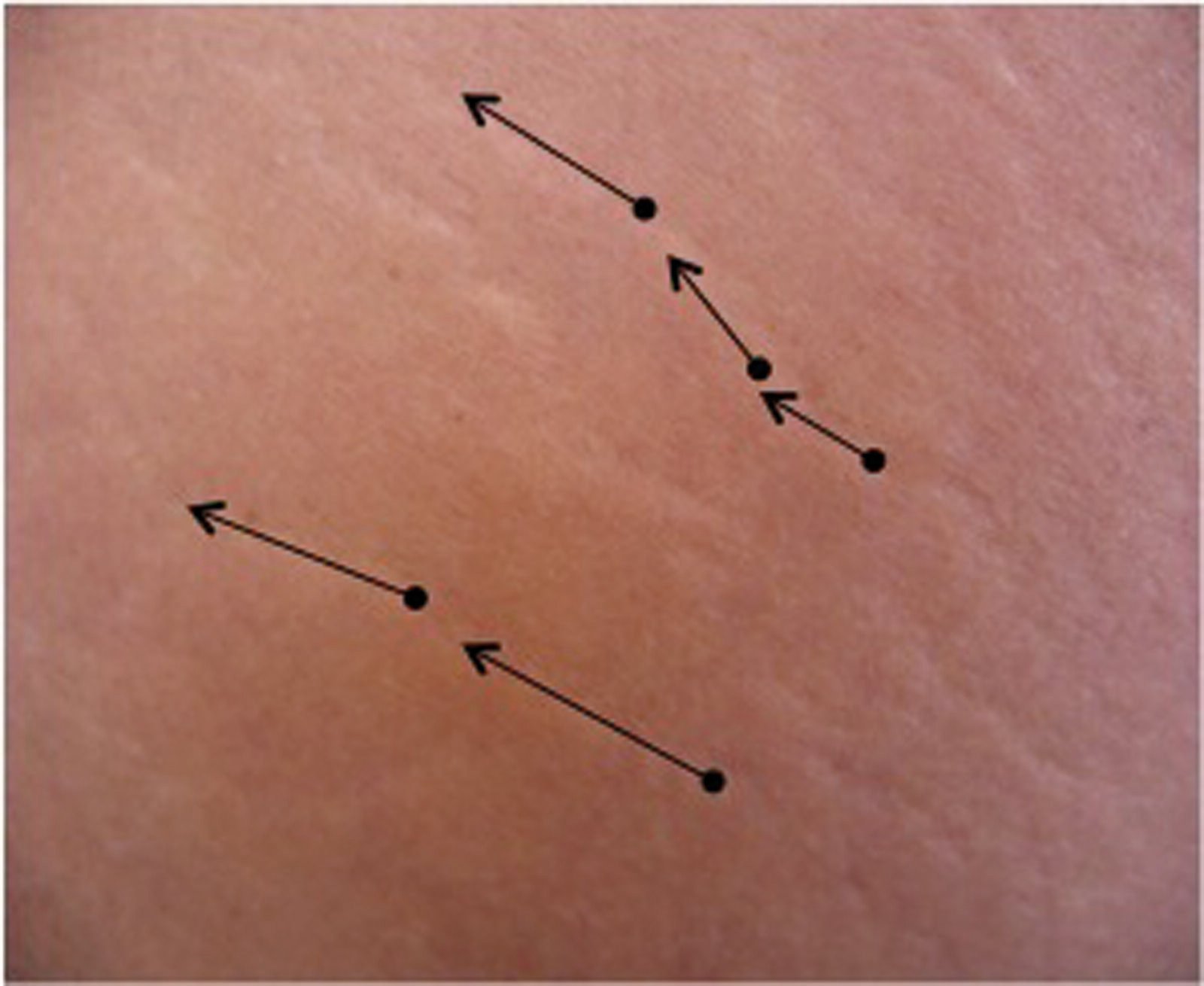
Figure 6 Detachment lines for stretch marks treatment
Stretch marks (striae atrophic, atrophy dermo–epidermal striae) are injuries caused by the shredding of the dermis and epidermis. They appear like linear scars and their origin are related to breakage of the collagen fibres, which occurs when the tissue is not sufficiently elastic, and to ischaemic damage owing to distension of the dermal capillaries.
Their occurrence is likely related to both mechanic (i.e. weight loss) and hormonal factors (i.e. steroid therapy), while the existence of a genetic predisposition is not clearly demonstrated.
The positive effects of CO2 therapy on the blood flow and oxygenation of peripheral tissue contributes to reduce the hypoxic damage, which is related to the aetiology of stretch marks. Histological examinations performed after treatment with CO2 showed that it modified, treatment by treatment, the structure of the dermis, inducing an increase in thickness and a more widespread distribution of collagen fibres 8.
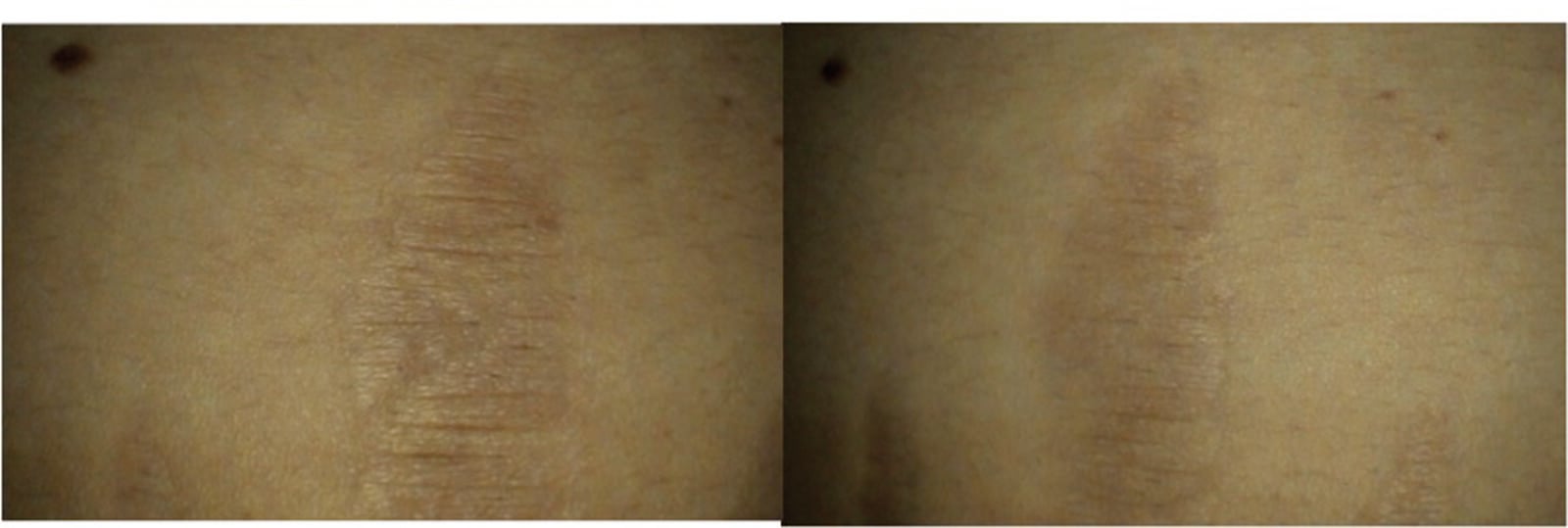
Figure 7 Stretch marks in a 44-year-old patient (left). Results after eight treatments (right)
Figure 6 shows the insufflation technique and Figure 7 shows the result obtained. The technique provides small infiltrations along the course of the stretch mark as shown in Figure 6, at the end of eight treatment sessions an improvement of skin quality can be noted (Figure 7).
Conclusions
Data in the literature makes it possible to conclude that CO2 therapy is a safe and useful treatment for a number of vascular diseases and skin affections.


