


Tertiary therapies
Chemical peels
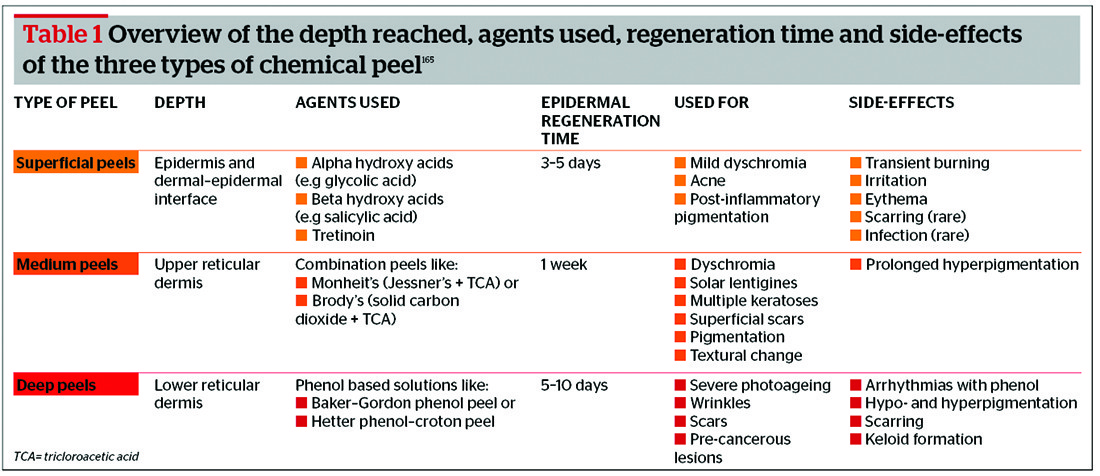
Chemical peels are an invasive procedure in which the skin layers are damaged, resulting in a controlled re-epithelisation, new collagen synthesis and evenly-distributed melanin. They are classified into superficial, medium-depth, and deep peels178. Their penetration depends on the substance, concentration and pH used during application, and the choice of these depends on the skin pathology being treated179 (Table 1). Chemical peels using phenol, salicylic acid, alpha hydroxy acid and trichloroacetic acid have all been used to treat photodamaged skin. Superficial peels using glycolic acid (GA) have been shown to reduce fine lines, increase collagen thickness, and thus improve overall skin texture180. Another superficial peel using salycilic acid at 30% was found to improve pigmentation and reduce wrinkles181. In a study comparing GA and capryloyl salicylic acid (LHA), it was noted that 5–10% of LHA is as effective as 20–50% of GA in improving hyperpigmentation and reducing fine wrinkles182.
Botulinum toxins
Botulinum toxin A (BoNTA) is naturally produced by Clostridium botulinum. Since 2002 it has been approved by the FDA to treat glabellar lines, following the results of a large double-blind, randomised placebo-controlled trial183. BoNTA does not reverse the effects of photodamaged skin, but simply and safely reduces wrinkles by reversibly paralysing treated muscles184. The dose depends on the muscle size; in fact, men usually require higher doses. In the glabellar region the effects of BoNTA last for approximately 4–6 months185, 186. In 2000, BoNTB was approved by the FDA for the treatment of cervical dystonia. It is not currently approved for cosmetic use, but has been used in an off-label fashion in this regard187, 188; a study by Baumann et al189 showed that it was safe and effective for the correction of crow’s feet. There seem to be no significant differences between BoNTA and B in treating forehead wrinkles, with BoNTA having a longer duration and BoNTB having a faster improvement rate186. Both BoNTA and B seem effective at 1 : 70 and 1 : 100 potency with no difference between the two potencies186.
Dermal fillers
Soft tissue augmentation or dermal fillers are used to reverse the volume loss in the face190. There are autologous fillers made from human fibroblasts, hyaluronic acid (HA), and synthetic or pseudo-synthetic fillers such as silicone. HA fillers are commonly used as they are safe, have low immunogenicity and are easily reversible with hyaluronidase190. Their effects last between 3 and 12 months191. Studies have shown that they increase skin’s hydration and fibroblast activation, leading to expression of collagen type I, MMP-1 and TIMP-1192, 193.
Calcium hydroxylapatite (CaHA) is a long-lasting, non-permanent dermal filler suspended in a sodium carboxymethylcellulose gel carrier194. The CaHA microspheres stimulate collagen formation around them, leading to a thickening of the dermis over time191. It is eliminated via the renal system and has been found to have low antigenicity and minimal inflammatory response. No cases of osteogenesis have been reported with this type of filler195.
Injectable poly-L-lactic acid (PLLA) is a synthetic biodegradable polymer that corrects bony and soft tissue facial deficiencies by producing a gradual increase in volume. It was approved for cosmetic use by the FDA in 2009196. Collagen deposition is stimulated through an inflammatory tissue response197. Among the rare and few side-effects noted are subcutaneous indurations and deep, minimally-visible multiple granuloma-like nodules198. Results are significant and long-lasting. Corrections can be maintained for up to 3 years with additional sessions199. Those with advanced volume loss and poor skin integrity may require more product and treatment sessions196.
Visible light devices
Ablative and non-ablative laser systems have been found to reverse some of the effects of photodamage, but to a different degree200. Ablative lasers act on both the epidermis and dermis and include CO2 and Er:YAG devices. Although the CO2 laser is effective at reducing wrinkles and scars, and improving skin tone, it has higher morbidity than the Er:YAG200. Complications with CO2 lasers include scarring and prolonged erythema. Na et al201 applied PRP after CO2 laser and found that PRP lessened some of the side-effects, and increased wound healing and collagen thickness. In another independent study it was observed that PRP plus laser increased skin elasticity, collagen and the number of fibroblasts202.
Non-ablative laser, fractional resurfacing and intense pulsed light (IPL) were developed to reduce the healing time and the patient’s discomfort by stimulating new collagen formation without causing epidermal disruption203, 204, and have become one of the most popular methods205. Some of these include Nd:YAG (1064 nm and 1320 nm), pulsed dye laser (PDL; 585–595 nm), diode (1450 nm), Er:Glass (1450 nm) and IPL (500–1200 nm)205. El-Domyati et al206 showed that multiple sessions with a fractional Er:YAG laser was as effective as a single session of ablative Er:YAG laser on increasing collagen, but not as effective on elasticity and epidermal thickness. When an Nd:YAG (1064 nm) laser was used as an ablative laser and compared with CO2 and Er:YAG, the results showed that apart from hyperpigmentation, side-effects were considerably less207. There are contradictory results with the 1450 nm diode; in one study significant improvement in dermal collagen was observed histologically208, and in another independent study only two out of 25 dermatologists could note any improvement209.

