


A triple-wavelength diode laser protocol combining 810, 940 and 1060 nm demonstrates promising improvements in skin tone, texture and wrinkles, with strong safety and high patient satisfaction in a small clinical study
Photo-ageing and chronological ageing primarily manifest as skin deterioration. This process is accelerated by intrinsic factors, including age and genetics, as well as extrinsic factors such as sun exposure, diet, and health habits. Common symptoms include a decline in skin texture and hydration, irregular pigmentation, wrinkle formation, and reduced elasticity1. Laser technologies are commonly used to treat conditions associated with skin ageing. The main objective is to utilise the absorption of light by specific chromophores to generate heat and trigger biological responses.
Non-invasive and non-ablative lasers emit light at specific wavelengths that are selectively absorbed by melanin, water, and haemoglobin chromophores to heat the skin. The use of a single wavelength provides specific penetration and targeted absorption of energy, which is employed primarily in treatments targeting a single chromophore, such as melanin, in hair removal2. Nevertheless, concerns have been raised regarding the safety of these treatments for individuals with darker skin types as well as their efficacy in addressing conditions that may require multiple wavelengths to target different tissue layers.
In high-powered diode lasers, two primary wavelength combinations are typically utilised: 755-810-1064 and 810-940-1060 nm. A number of studies involving hair removal have established the efficacy and safety of both combinations3-5. Nevertheless, the efficacy of these wavelengths in treating visible signs of ageing remains poorly studied, with only limited evidence available for the 755-810-1064 nm combination6.
The objective of this study was to investigate the safety and efficacy of a triple-wavelength diode laser system that combines 810, 940, and 1060 nm, using a protocol that integrates both long and short pulses to improve facial skin quality. To support these findings, COMSOL Multiphysics simulations were conducted to model the interactions between the laser energy and various layers of the skin.
Materials and methods
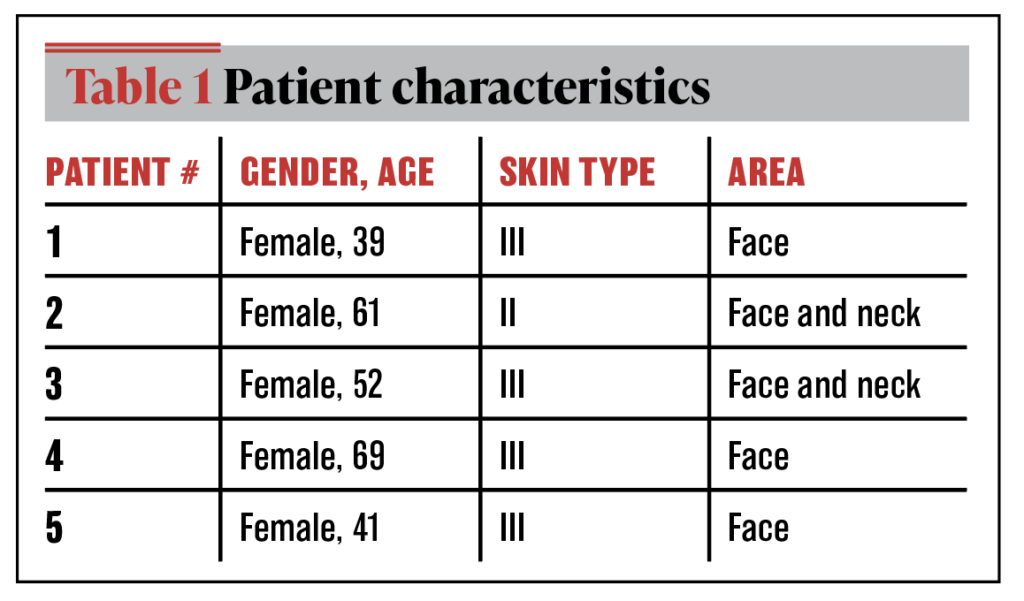
This small sample size retrospective study involved five Korean female patients aged between 39 and 69 years, all of whom expressed concerns regarding their facial appearance, tone, and texture (Table 1). The cohort was comprised of healthy individuals with no contraindications commonly associated with diode laser treatment. The participants were treated at Clinique Hus, Hu (Seoul, South Korea) and provided informed consent before the procedure.
Patients underwent one to four treatments at 1-month intervals, utilising the Primelase Excellence® (Sinclair; Barcelona, Spain) 4,800 W diode laser, the triple-wavelength Blend handpiece (810, 940, and 1064 nm), and a spot size of 20 mm x 9 mm. The treatment protocol was designed specifically for the device and handpiece.
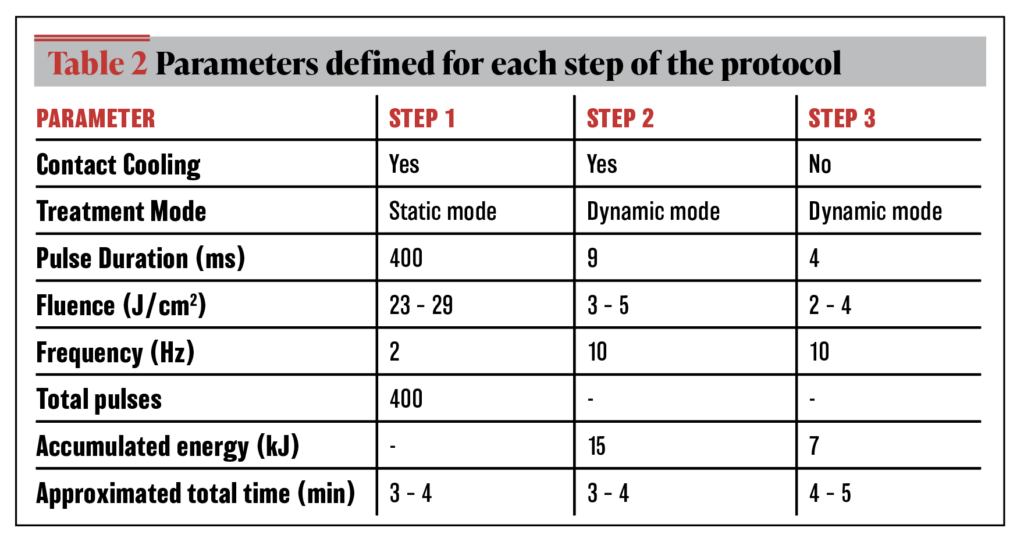
The treatment protocol comprised three stages targeting the cheeks and neck, with 75% of the total treatment time allocated to the cheeks and 25% to the neck. The treatment parameters used in each step are listed in Table 2.
- Step 1: A static mode with long pulses of 400 ms at high fluence was employed to achieve deep-tissue heating with additional skin contact cooling. Slow sweeping movements were performed to cover the entire treatment period, ensuring the completion of the predefined number of pulses.
- Step 2: Dynamic mode with short 9 ms pulses at low fluence, combined with skin-contact cooling, was employed to heat the dermis and raise the hair follicle temperature. Rapid sweeping movements were applied across the entire treatment area until the designated treatment time elapsed, and the specified energy was fully delivered.
- Step 3: A dynamic mode with 4 ms short pulses at low fluence was used for a fast-sweeping movement without skin cooling. This step aimed to superficially heat the dermis while maintaining the hair follicle temperature above 50°C. Rapid sweeping was conducted across the entire study area. However, the lack of skin cooling can result in excessive heat. An infrared thermometer was used to monitor the skin temperature and, if it exceeded 42°C, the treatment was paused for 20 seconds to allow the skin to cool. The treatment was continued in an alternating sequence of pulse applications and pauses until the required accumulated energy was delivered.
The treatment sessions were conducted by a single physician, Kyungkook Hong. High-resolution photographs were obtained using the Visia® and Vectra® imaging systems (Canfield Scientific, Inc.; Parsippany, NJ, USA).
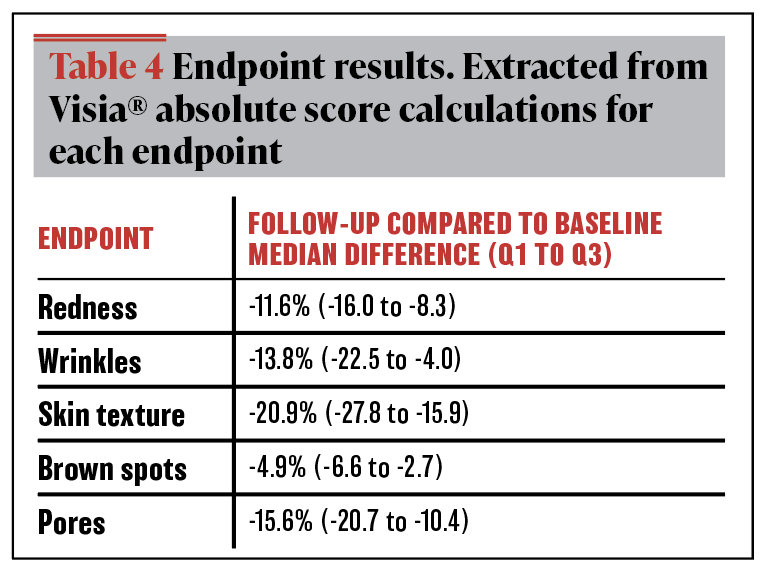
Skin quality was assessed using an objective score obtained using the Visia® system. The system was used 3 months after two treatment sessions to quantitatively evaluate changes in redness, wrinkles, skin texture, brown spots, and pore size. This system has been previously validated to provide objective clinical data7. The results are presented as medians and interquartile ranges (IQRs).
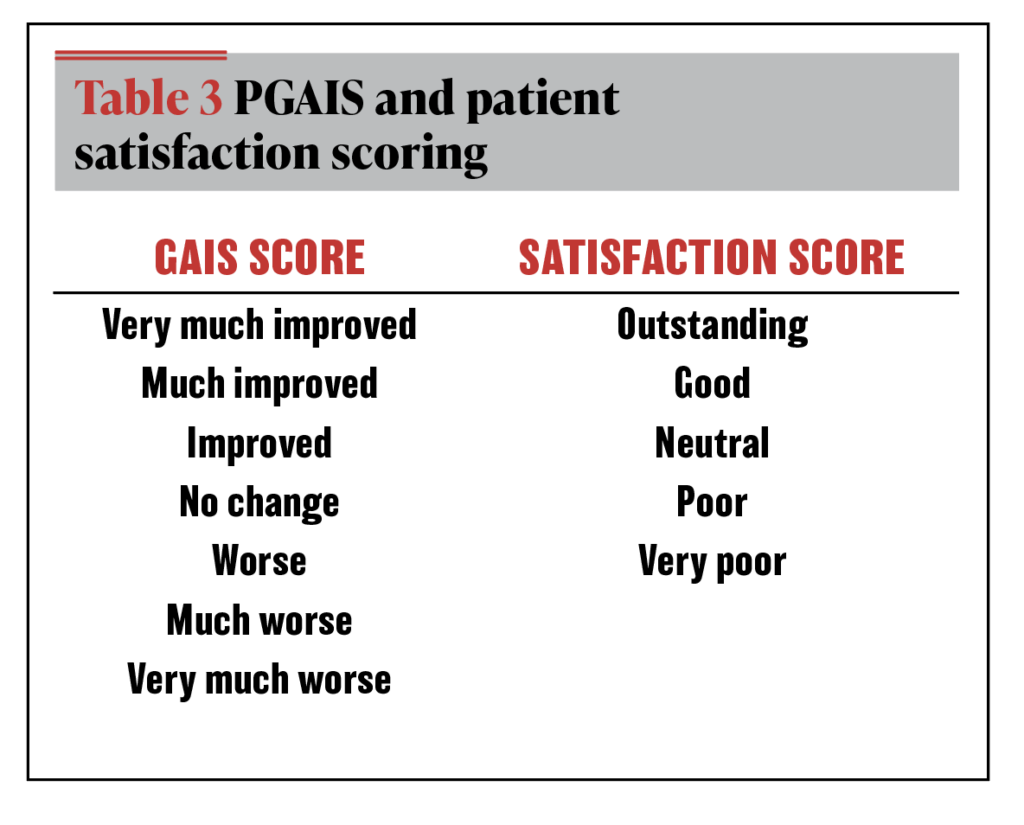
The Vectra® imaging system was used in follow-up sessions to evaluate overall aesthetic clinical efficacy and facial contour, with GAIS (Global Aesthetic Improvement Scale) scores recorded by two experienced physicians. Patients’ pain levels and incidence of adverse effects were documented at each treatment session and follow-up appointment. Patient satisfaction was recorded at the end of the follow-up session using the scale presented in Table 3.
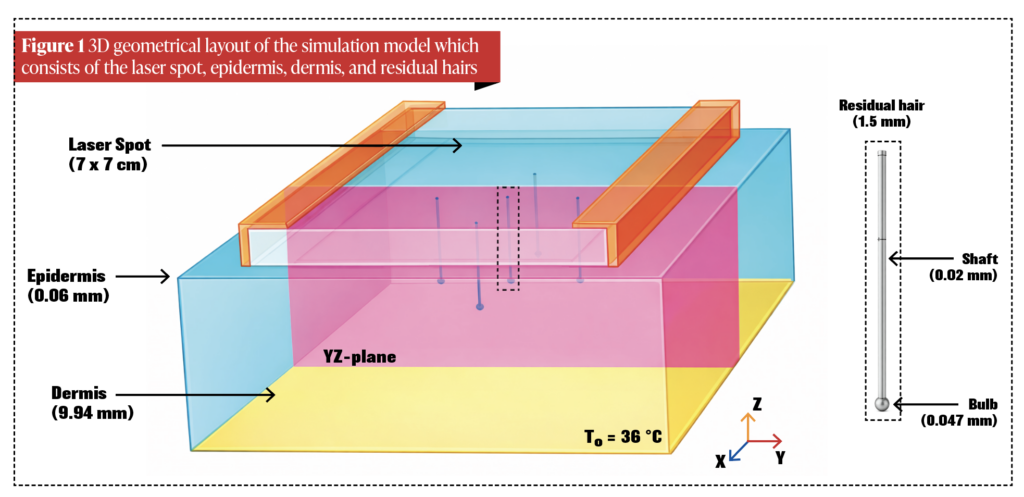
A realistic 3D model was created using COMSOL Multiphysics® software (version 6.0, COMSOL Inc.; Burlington, MA, USA) to simulate the effects of the treatment protocol on skin tissue. The geometry consisted of a sapphire laser spot surface, biological tissues (epidermis and dermis), and residual hair in the centre of the tissue (Figure 1). The scientific foundation of this simulation was consistent with that of a previous study that modelled the performance of the same diode laser handpiece for hair removal8.
Several modifications were made in the current study to ensure alignment with the defined protocol:
- The wavelength utilised in this study was a simultaneous combination of 810, 940, and 1060 nm
- The laser spot size and energy were adjusted to 7 cm x 7 cm to simulate movement and energy accumulation during the treatment. The energy applied at each step accounted for 75% of the total treatment energy to simulate treatment of the cheek area, excluding the neck, with a single conversion of the equivalent energy delivered for a 7 cm x 7 cm spot
- The three steps of the protocol were simulated continuously, with a 35s pause time between steps and a total treatment time of 10 min
- Residual hair was included in the model
- Blood perfusion and heat flow between the epidermis and dermis were simulated during pauses between the stages of the protocol.
Results
In addition to the anticipated adverse effects, including mild-to-moderate erythema and slight post-treatment oedema, which dissipated within a few hours, no significant adverse events were observed in any patient. The patients reported experiencing mild-to-moderate pain during treatment. Figure 2 illustrates the Visia® photographs of the patients before and 3 months after two treatment sessions, illustrating changes in the assessed endpoints, including redness (a–b), wrinkles (c–d), skin texture (e–f), brown spots (g–h), pores (i–j) and Vectra® images obtained before treatment and during follow-up sessions (k–l). Visia® analysis was not conducted for Patient 1. These images facilitate the assessment of the overall facial changes and contours. Table 4 presents the results for the clinical endpoints, given the small sample size.
The overall aesthetic clinical effectiveness, using the GAIS scale at follow-up, was assessed as ‘improved’ and ‘very improved’ compared with baseline in 40% and 60% of patients, respectively. All patients reported satisfaction with the results as ‘good’ (60%) or ‘outstanding’ (40%).
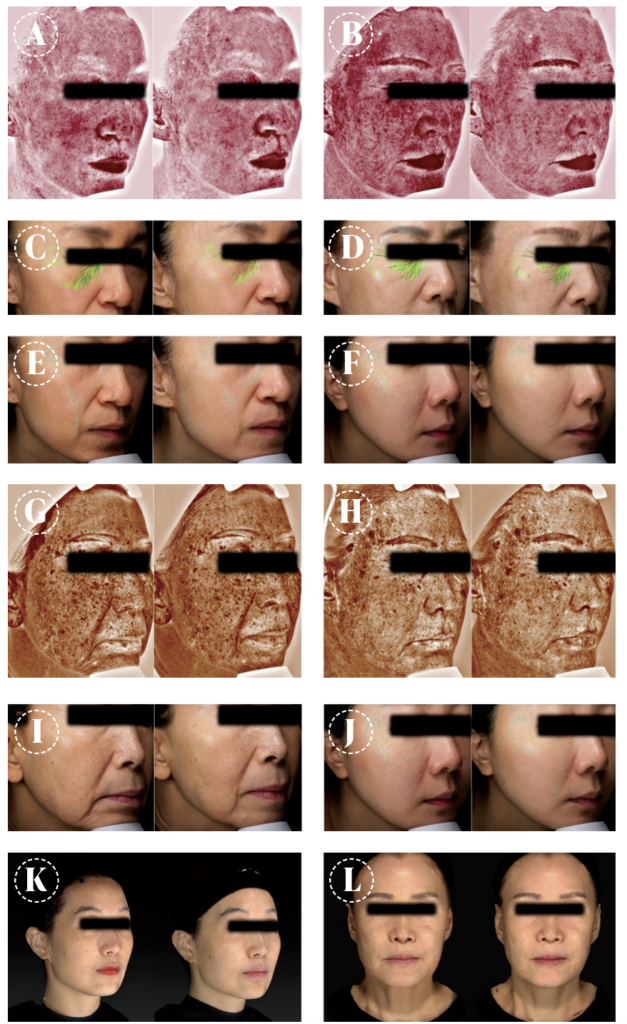
Figure 2: Before and after results with Visia (a–j) and Vectra (k–l). (a) Patient 2 (P2), redness -22.2%; (b) P4, redness -13.9%; (c) P2, wrinkles -22.2%; (d) P4, wrinkles -23.3%; (e) P2, skin texture -17.4%; (f) P1, skin texture -37.8%; (g) P3, brown spots -0.0%; (h) P4, brown spots -7.9%; (i) P3, pores -13.5%; (j) P1, pores -29.9%; (k) P5, 1 session, follow up 4 months, GAIS ‘much improved’; (l) P4, 4 sessions, follow up 6 months, GAIS ‘much improved’.
Simulation results
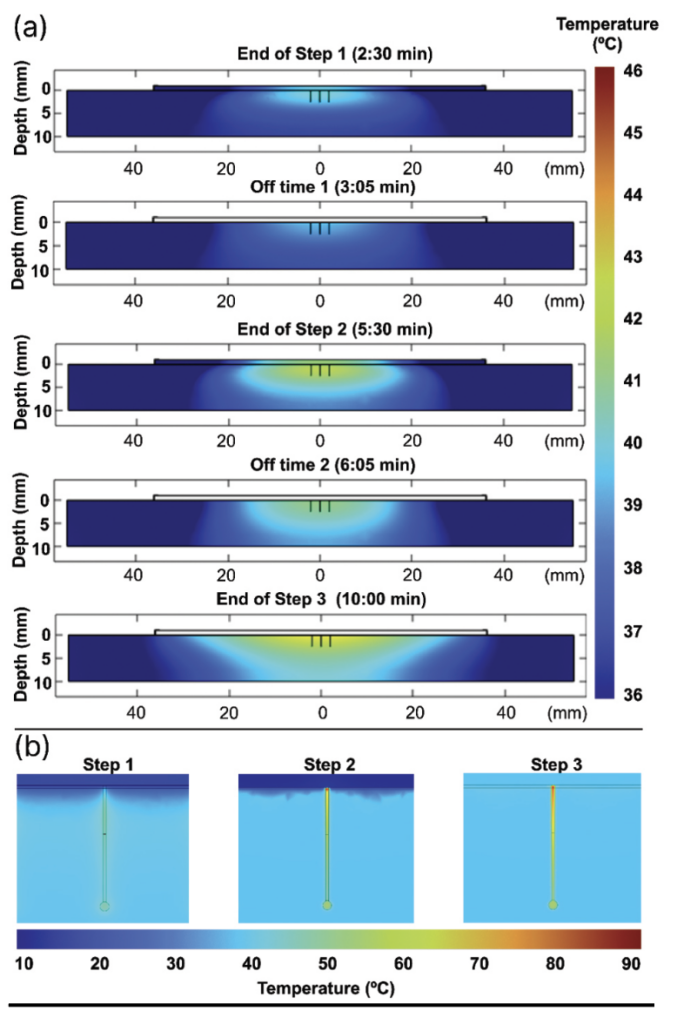
Figure 3 illustrates the simulated distribution of temperature in the skin at the end of each step and during the 35-s pause in the protocol, as well as the heat distribution into the residual hair from a single pulse at each step.
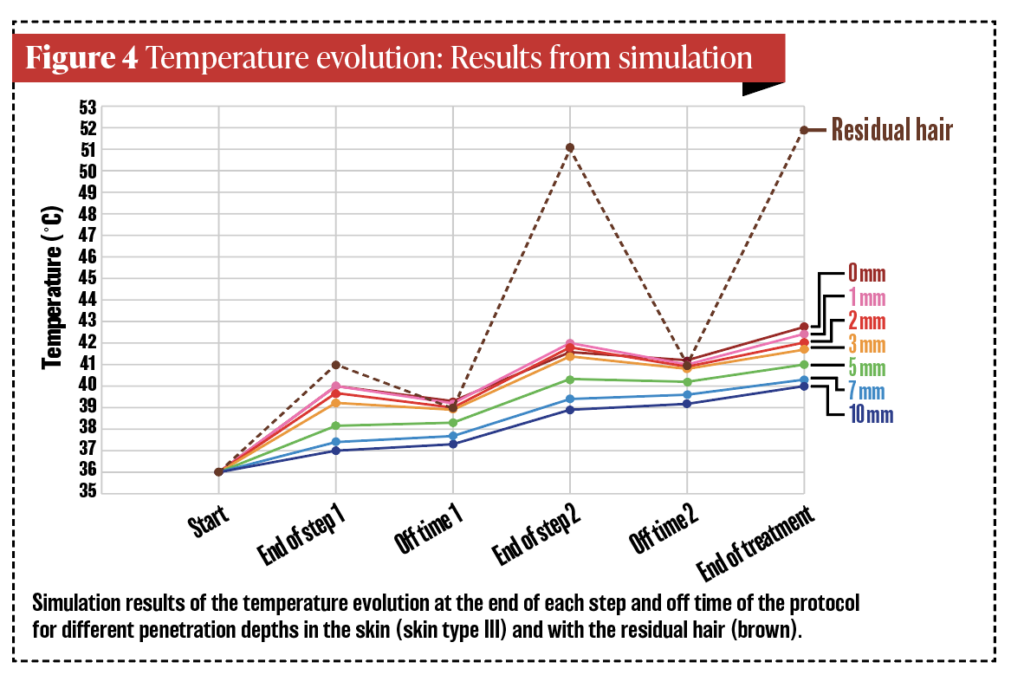
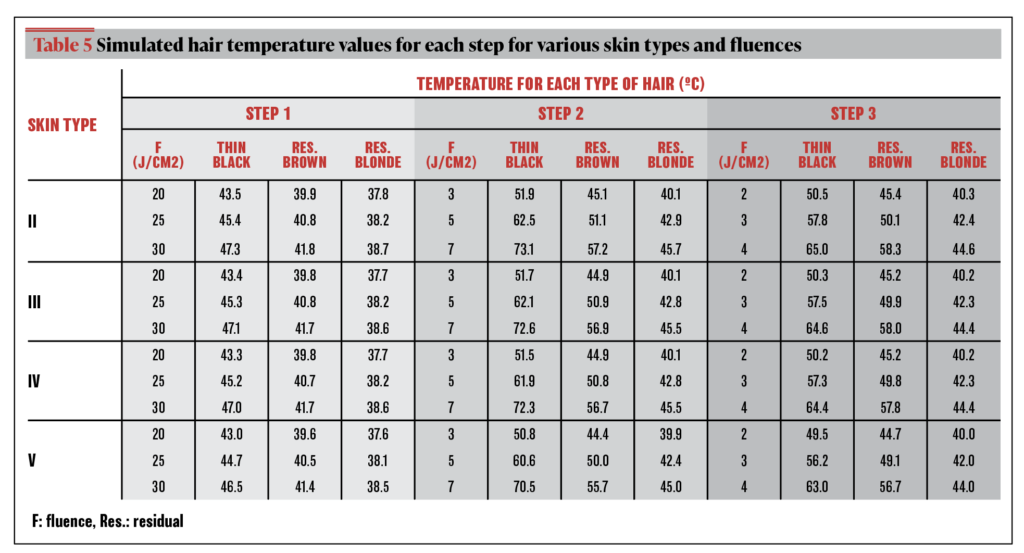
Figure 4 shows the simulated temperature progression at various tissue depths at the end of each treatment step, along with the protocol’s pause times. Table 5 lists the temperatures of the different hair types simulated at each of the three steps for varying skin types.
Discussion
The objective of this study was to assess the efficacy and safety of a novel diode laser device with a combination of wavelengths (810, 940, and 1060 nm) in a small cohort of patients to improve the appearance, texture, and tone of the skin. Five patients were treated, and the results suggest that the protocol offers promising outcomes. The use of multiple wavelengths in conventional hair removal treatments has not been sufficiently explored. The application of this device for global skin improvement remains poorly researched9.
As stated by Park et al.10, the four most common skin quality problems in Asia are uneven skin tone, skin surface irregularity, skin laxity, overactive sebaceous glands, and enlarged pores. Our results indicate a notable reduction in facial redness, with a median change of -11.6% (IQR -16.0 to -8.3), as illustrated in Figure 2 (a–b). Facial redness and telangiectasia are common dermatological conditions that can negatively affect skin appearance. Conventional lifting devices have proven to be ineffective in addressing these issues. However, the absorption of 940 nm by haemoglobin enabled the Primelase Excellence® Blend handpiece to potentially improve facial redness and telangiectasia.
A reduction was observed in the depth and visibility of wrinkles, including both fine and deep wrinkles (Figure 2 c–d), with a median reduction of -13.8% (IQR -22.5 to -4.0). This suggested that the temperatures necessary to stimulate collagen production were attained, resulting in a more uniform and youthful complexion, consistent with the simulation findings. Furthermore, a notable improvement in skin texture (-20.9%) was observed (IQR -27.8 to -15.9), as illustrated in Figure 2 (e–f). Additionally, a -15.6% (IQR -20.7 to -10.4) reduction in pores was noted, as shown in Figure 2 (i–j). These changes suggest a trend towards a more uniform and healthier skin appearance, which can lead to improvements in patient self-perception and satisfaction. However, given the small sample size (N=5), the generality of these findings is limited, and caution should be exercised when interpreting the results. These findings are comparable to those obtained using alternative technologies such as diode lasers11, 12.
A remarkable finding of the study was the reduction in brown spots and skin pigmentation by -4.9% (IQR -6.6 to -2.7), as shown in Figure 2 (g–h). This finding suggests that the high-wavelength combination did not worsen pigmentation issues such as melasma, nor did it provoke post-treatment hyperpigmentation. Rather, it appears to have improved skin tone. The safety of pigmentation management helps in determining the most appropriate procedures for patients with sensitive skin or a history of altered pigmentation. These results can be compared with those obtained using other laser diode technologies9, 13.
Implementation of this protocol resulted in a noticeable improvement in skin appearance in all treated patients. GAIS scores were ‘improved’ or ‘very much improved’ in all treatments. Improvements were visible from the first treatment session (Figure 2 k–l) but became more pronounced after 2–4 sessions. The protocol was safe, with no serious or permanent adverse effects. The most common adverse effects were mild to moderate pain and transient erythema, indicating that this technique was well tolerated. Patient satisfaction scores were ‘good’ and ‘outstanding’ for all patients. Patient satisfaction was higher than the GAIS score of doctors, which may be because patients valued the resolution of visible signs of photodamage and ageing more than physicians when assessing clinical endpoints.
In addition to employing combined wavelengths (810, 940, and 1060 nm), the protocol incorporated high fluences with long pulses and low fluences with short pulses in various stages. Multiphysics simulations provided insights into the thermal effects of these parameters on different skin structures and depths, as illustrated in Figures 3–4. Simulations have been employed to illustrate the thermal distribution of other technologies with different applications, such as cryolipolysis14 and treatments for skin improvement, including radiofrequency15. Furthermore, the simulations illustrated the efficacy of the diode laser in this protocol for hair removal, demonstrating its effectiveness and safety on dark skin5, 8.
The use of high fluences and long pulses in the initial phase of the protocol led to a general elevation in skin temperature to approximately 40°C at a depth of up to 3 mm (Figure 4). This effect was due to the absorption of the 940 and 1060 nm wavelengths by water and haemoglobin in the tissues, respectively, without excessive heating of the residual hair. In the second step, a combination of lower fluences and short pulses resulted in an overall increase in tissue temperature to approximately 42°C and an elevation in the temperature of residual hair to 51°C. Short pulses, which are shorter than the thermal relaxation time of the hair, combined with the 810 nm wavelength that targets melanin in the hair, produce this effect. The increase in temperature creates a thermal environment around the hair of over 50°C, which may promote collagen fibre contraction and denaturation16, resulting in enhanced skin contraction and remodelling. The first two steps of the protocol included contact cooling of the applicator tip, which prevented a significant increase in the skin temperature. This finding correlates with the mild pain reported by the patients and their ability to tolerate treatment without compromising the targeted tissue temperatures.
In the final stage of the protocol, a shorter pulse and lower fluence were used without contact cooling. This resulted in an increase in surface skin temperature and a further rise in internal tissue temperature to over 42°C, with hair temperature reaching 52°C. Figures 3 and 4 illustrate that by the end of the treatment, uniform heating of the target area was achieved, with temperatures ranging from 40 to 43°C at a depth of 7 mm. These temperatures promote long-term collagen remodelling and neocollagenesis and induce the release of growth factors, cytokines, and members of the heat shock protein (HSP) family16, 17.
Controlled and selective heating of hair is of paramount importance for the implementation of this protocol. Heating hair to temperatures exceeding 50°C is expected to result in shrinkage and denaturation of collagen in the surrounding tissue, thereby enhancing treatment efficacy. Table 5 lists the simulation results for various hair types. As expected, blonde hair, which has a lower melanin content, underwent less heating than fine black hair, which reached significantly higher temperatures. These simulations provide valuable insights and show that it is essential to adjust the treatment parameters to achieve a balance between selective hair heating and overall skin heating without causing damage. When the skin is heated homogeneously, combined with high temperatures around the hair, a thermal needling effect (TNE) is produced, which is comparable to that achieved with other technologies such as micro-focused ultrasound or fractional lasers. However, the TNE approach avoids the complications associated with these more invasive techniques11, 12.
The main limitation of this study was its small sample size (N=5). Future research should include a larger and more diverse patient population to validate these findings and explore the effect of treatment on different skin types, including male skin with thicker facial hair.
Conclusions
The findings of this study suggest that the use of multiple-wavelength laser diodes may be an effective method for improving skin appearance and achieving greater uniformity in skin colour and texture. Furthermore, the combination of high fluence with long pulses and low fluence with short pulses appears to result in immediate contraction and denaturation of skin collagen fibres, while also providing long-term stimulation of new collagen production. The use of multiphysics simulations has enhanced our understanding of the energy distribution in the skin, thereby expanding the potential applications of laser diodes beyond their conventional use in hair removal.
- Declaration of interest This study received no external funding.
- Ethics StatementAll study procedures were conducted according to the Declaration of Helsinki. The authors confirm that ethical review committee approval is not necessary as the study device is already FDA-approved and CE-marked. The device was used in accordance with the parameters of use validated by these authorities and in line with local standards. All participants were fully informed about the procedures and gave informed consent before participation.
- Data Availability StatementThe datasets generated during and/or analysed during the current study are available from the corresponding author upon reasonable request due to patients’ privacy reasons.
References
- M. Yaar and B. A. Gilchrest, “Photoageing: Mechanism, prevention and therapy,” Nov. 2007. doi: 10.1111/j.1365-2133.2007.08108.x.
- S. D. Gan and E. M. Graber, “Laser hair removal: A review,” Jun. 2013. doi: 10.1111/dsu.12116.
- E. P. Raj Kirit, A. Sivuni, S. Ponugupati, and M. H. Gold, “Efficacy and safety of triple wavelength laser hair reduction in skin types IV to V,” J Cosmet Dermatol, vol. 20, no. 4, pp. 1117–1123, Apr. 2021, doi: 10.1111/jocd.13995.
- M. H. Gold et al., “Safety and efficacy for hair removal in dark skin types III and IV with a high-powered, combined wavelength (810, 940 and 1060 nm) diode laser: A single-site pilot study,” J Cosmet Dermatol, vol. 21, no. 5, pp. 1979–1985, May 2022, doi: 10.1111/jocd.14926.
- A. Pall and G. Viera-Mármol, “Triple Wavelength and 810 nm Diode Lasers for Hair Removal: A Clinical and in Silico Comparative Study on Indian Skin,” Journal of Cosmetics, Dermatological Sciences and Applications, vol. 12, no. 04, pp. 164–173, 2022, doi: 10.4236/jcdsa.2022.124014.
- J. Y. Jo, D. H. Suh, H. Park, S. J. Lee, and H. J. Ryu, “Skin rejuvenating effect of a combined triple-wavelength (755 nm, 810 nm, and 1064 nm) laser: a preliminary study,” Lasers Med Sci, vol. 38, no. 1, Dec. 2023, doi: 10.1007/s10103-023-03936-6.
- H. Henseler, “Validation of the Visia ® Camera System for for skin analysis through assessment of the correlations among the three offered measurements – the percentile, feature count and absolute score – as well as the three capture perspectives, from the left, front and right,” GMS Interdisciplinary Plastic and Reconstructive Surgery, vol. 11, 2022
- G. Viera Mármol and J. Villena, “New 3D in silico model of hair and skin heating during laser hair removal,” Interna-tional Research Journal of Pharmacy and Medical Sciences (IRJPMS), vol. 1, no. 1, pp. 15–24, 2019.
- N. Voravutinon, K. Seawthaweesin, A. Bureethan, A. Srivipatana, and P. Vejanurug, “Efficacy of diode laser (810 and 940 nm) for facial skin tightening,” 2015.
- J.-Y. M. Park, J.-F. M. Chen, H. M. Choi, and wilson W. S. Ho, “Insights on Skin Quality and Clinical Practice Trends in Asia Pacific and a Practical Guide to Good Skin Quality from the Inside Out,” Journal of Clinical and Aesthetic Derma-tology, vol. 15, no. 6, pp. 10–21, 2022, [Online]. Available: https://www.researchgate.net/publication/361799484
- N. Saedi, K. Petrell, K. Arndt, and J. Dover, “Evaluating facial pores and skin texture after low-energy nonablative frac-tional 1440-nm laser treatments,” J Am Acad Dermatol, vol. 68, no. 1, pp. 113–118, Jan. 2013, doi: 10.1016/J.JAAD.2012.08.041.
- J. Y. Park, S. Youn, W. Hong, K. C. Lee, and I. Kim, “Treatment Protocol on Using Microfocused Ultrasound with Vis-ualization for Skin Quality Improvement: The Korean Experience,” Plast Reconstr Surg Glob Open, vol. 11, no. 5, p. e5029, May 2023, doi: 10.1097/GOX.0000000000005029.
- A. Koren et al., “Evaluation of subject response following treatment for pigmentation or wrinkles using a diode laser,” J Cosmet Dermatol, vol. 19, no. 6, pp. 1371–1376, Jun. 2020, doi: 10.1111/jocd.13200.
- G. Viera Mármol and J. Villena, “New Cooltech Define® Cryoadipolysis Applicators: A Scientific and Comparative Study with Cooltech® Applicators,” Eurasian Journal of Medical Investigation, vol. 3, no. 2, pp. 85–94, 2019, doi: 10.14744/ejmi.2019.35267.
- G. V. Mármol, A. L. U. Bojorge, A. R. Jorge, J. A. F. Martínez, and O. C. Lozano, “From Simulation to Reality: A Com-prehensive Study on the Efficacy of a Rotating Monopolar and Bipolar Radiofrequency System through <i>In-Silico</i> Modeling and Pre-Clinical and Clinical Validation,” J Biomed Sci Eng, vol. 17, no. 06, pp. 107–128, 2024, doi: 10.4236/jbise.2024.176009.
- L. Bozec and M. Odlyha, “Thermal denaturation studies of collagen by microthermal analysis and atomic force mi-croscopy,” Biophys J, vol. 101, no. 1, pp. 228–236, Jul. 2011, doi: 10.1016/j.bpj.2011.04.033.
- J. R. Macdonald and H. P. Bächinger, “HSP47 Binds Cooperatively to Triple Helical Type I Collagen but Has Little Effect on the Thermal Stability or Rate of Refolding,” Journal of Biological Chemistry, vol. 276, no. 27, pp. 25399–25403, Jul. 2001, doi: 10.1074/jbc.M102471200.





{kind=link}