

Chedly Bouzouaya and Ronald Feiner describe a novel new technique to perform upper-lid blepharoplasty without any noticeable scars
Blepharoplasty is one of the most commonly performed facial cosmetic procedures today. It remains an elective operation and should be performed by well-trained experienced surgeons to avoid any potential complications. Even with experienced surgeons, the most frequent complications seen are excessive or insufficient skin removal, an abnormal lid crease, and frequently a noticeable scar. The authors concur with Flowers’ dictum that 20 mm of anterior lamella is necessary for normal functioning of the upper-lid1.
Traditionally, upper-lid blepharoplasty approaches have been constrained by the insistence of many surgical strategists that any brow ptosis contribution to lid redundancy should be addressed first. However, with the success of minimally invasive injectable forehead botulinum toxin and filler therapies, invasive surgical browlifts are now often unnecessary.
Furthermore, surgical brow lifts have been associated with risks factors such as bleeding, nerve damage, scarring, alopecia, brow asymmetry and over/under elevation2–4.
Contemporary innovations in cosmetic surgery are generally hallmarked by a trend towards a deconstruction of aggressive operative techniques. Patients seek natural outcomes, intolerant of the stigmata associated with an overly ‘operated-on’ appearance, and fast recovery. This is a challenging brief for the surgeon. However, very pleasing outcomes can be achieved without visible scars and without recourse to invasive surgery.
The Chedly ‘C’ approach
Building on past innovations, the ‘Chedly C’ design provides for elegant eyelid enhancement. The technique has been designed in accordance with contemporary principles, incorporating several other preceding innovations devised by the authors.
This latest innovation is artistic but without entrapment into unnecessary complexity. The skin incisions are made in the patient’s natural eyelid crease with lateral extension visually muted by the author’s ‘C’ design. The ‘Chedly C’ construct avoids the common nuisance of the incision scar extending laterally to and frequently beyond the orbital rim.
This technique further advances the objective of achieving an aesthetically pleasing, elegant upper blepharoplasty outcome.
Technique
Traditionally, most textbooks and clinical papers describe the incision in the lid crease as a line which begins above the upper punctum, extends to the lateral canthus and then slopes upward 5 to 6 mm above the canthal angle in one of the lateral canthal creases, about 1.5 cm beyond the lateral canthus (or more depending on the lateral hooding). Beyond the lateral canthal angle, one encounters orbital rather than lid skin5.
However, orbital skin is much thicker than upper eyelid skin and tends to heal with a more noticeable scar6.
The technique we describe here removes only eyelid skin and the incision is hidden in the lid crease all the way from medial to the lateral aspect of the upper eyelid.
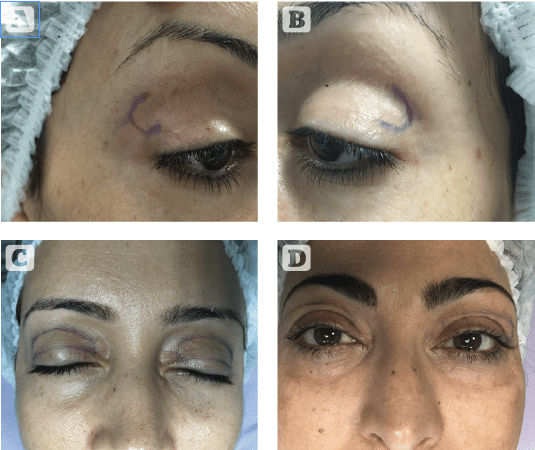
Figure 1 (A) ‘C’ drawing right eye (B) ‘C’ drawing left eye (C) completed ‘C’ drawing eyes closed.
(D) completed ‘D’ drawing eyes open. No lateral redundant skin
Pre-operative evaluation should record in detail any associated eyelid deformities. The amount of excess eyelid skin is estimated while the patient is in the upright position as it appears considerably less when the patient is supine. The marking of the lateral hooding of the skin is then addressed. The patient is prone, and the lower incision line is marked within the eyelid crease if present or at the planned new crease position 10 to 12 mm above the central eyelid margin.
During the pre-operative evaluation, we gently stretch the eyebrow and we indicate the upper eyelid crease site with a marking pen. This begins above the punctum. We ask the patient to look slightly upward; the marked line should fall into the upper eyelid crease that forms during a slight upward gaze. One blade of a smooth forceps grasps the centre marked line and the other blade grasp the skin superiorly, the forceps are reapplied until all redundant upper eyelid skin is eliminated, the lashes evert and the upper eyelid is elevated slightly from its closed position when the forceps meet. A mark is made centrally at the site of the upper forceps blade in this position; the procedure can be repeated nasally and temporally, a marking will connect these lines with the nasal and temporal end of the eyelid crease line. The marking is then extended medially and downward to 5 mm above the lid margin. Laterally the line should end at the canthal angle about 6 mm above the lid margin. From this point, a C shape incision line is marked upward toward the lateral brow. The width of the ‘C’ depends on the degree of temporal hooding. There is no extension in to the crow’s feet as is done traditionally (Figures 1–4).
With the C shape technique, there is no lateral extension no scar and a faster recovery.
Nasally a wide variety of techniques are used to allow skin removal and to prevent webbing, including removing a separate burrow’s triangle in this area. We have the incision in the medial portion in an upward position, and the orbicularis is resected so the skin without orbicularis will allow for an easy closure with no canthal webbing and no need for extra skin incision and extension of the scar beyond the lid crease.
As patients are considering upper lid Blepharoplasty at a younger age, there are no crow’s feet lines and no need in inducing one surgically.
The authors’ favour radiofrequency technology for all surgical tissue manipulation, including incision, dissection, resection, and control of bleeding. Radiofrequency technology will also result in a tissue mild contractive phenomenon, further securing a durable blepharoplasty outcome7–9.

Figure 2 (A) immediate post resection photos, without lateral extension,
(B) Immediate post surgical closure with continuous suture, without lateral extension
Conclusion
Less aggressive innovations in blepharoplasty surgery have facilitated natural outcomes with minimal trauma. To maintain the fidelity of our patients’ intrinsic appearance, incisions should be made in the patient’s natural eyelid crease. The skin sacrificed should be sufficient enough to remove almost all redundancy but cautious enough to ensure eyelid closure and avoiding iatrogenic lagophthalmos. The ‘Chedly C’ construct modifies the lateral upper lid incision by avoiding extension laterally to and beyond the orbital rim where scar formation is more evident and troublesome. The authors find patient acceptance and satisfaction is higher without the longer-term defect of a lateral orbital scar extension commonplace in upper blepharoplasty cases.
Declaration of interest None
Figures 1-2 © Bouzouaya


