

Discussion
Regenerative cell-based strategies, such as those encompassing the use of stem cells, hold tremendous promise for augmentation of the soft-tissue space23. Preclinical and published clinical studies show that ADSCs offer the possibility of finally fulfilling the key principle of replacing like for like as an aesthetic filler, without the drawbacks of the old methods of lipofilling. These drawbacks include an unpredictable degree of resorption of the transplanted fat and the need for multiple sessions of fat grafting in order to achieve the desired result.
Clinical studies on ADSCs, performed up to 2009, have not used a control group in order to objectively compare the SEL technique to the conventional lipografting. In 2011, the first study comparing autologous fat grafting to SEL was published15. A group of 20 patients with congenital or acquired facial tissue defects were included in this study and randomly divided into two groups. Ten patients were treated with autologous fat transplantation, and the remaining ten were treated with adipose-derived stem cell-enriched lipografts. Stromal enriched lipografts produced superior results without the need for repeat treatment sessions, which were necessary with autologous fat transplantation.
The presence of adipose-derived stem cells in adipose tissue transplantation may contribute to neoangiogenesis in the acute phase by acting as endothelial progenitor cells or angiogenic factor-releasing cells13. In vivo, ADSCs demonstrate the capacity to proliferate in response to a hypoxic insult remote from their resident niche, and this has been supported by in vitro studies showing increasing ADSCs proliferation with greater degrees of hypoxia25. The number of functional ADSCs is likely to be important for tissue repair, remodelling, and ADSC differentiation into vascular endothelial cells that contribute to neoangiogenesis in the acute phase of transplantation. ADSCs also up-regulate their pro-neovascular activity in response to hypoxia, and may harbour the capacity to find ischaemic tissue and function cooperatively with existing vasculature to promote angiogenesis26.
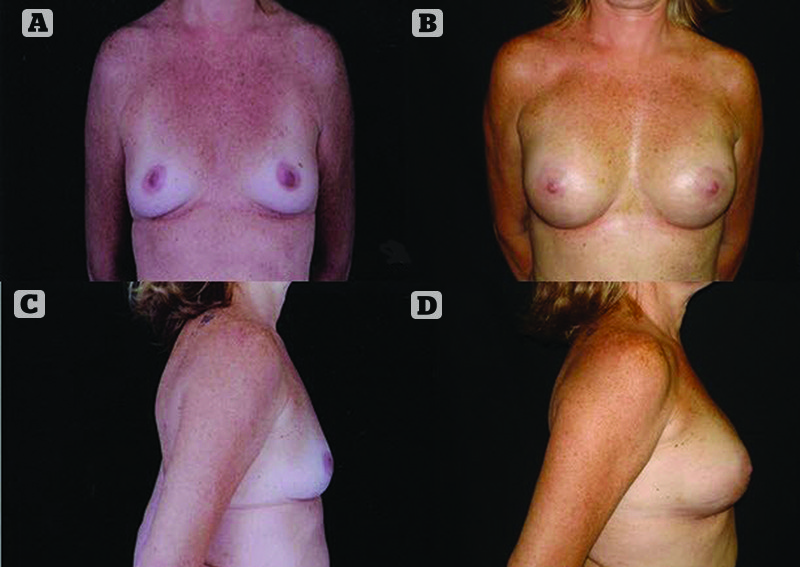
Figure 4 (A) and (B) Preoperative photos of a 32-year-old woman requesting breast augmentation, and (C) and (D) postoperative photos after breast augmentation by stromal enriched lipograft
Considerations for future use
The role of platelet-rich plasma (PRP) combined with autologous fat transplantations has been the subject of ongoing research. Positive effects of PRP and angiogenesis favouring processes, and proliferation of ADSCs have been demonstrated experimentally27.
In two human studies, PRP-assisted lipotransfer was used in breast augmentation compared with lipotransfer only. In a recently published study, the patients treated with PRP combined with autologous fat grafts showed a 69% maintenance of the breast contour 1-year postoperatively, while the patients of the control group treated with centrifuged fat grafting showed a 39% maintenance28. However, a different study revealed that fat grafting plus PRP was not superior to centrifuged fat grafting alone and the rate of liponecrosis at breast ultrasound was similar in the two groups29. A comparative study of platelet-rich fibrin (PRF) and PRP use in combination with fat grafting suggested that the combination of fat and PRF was more effective than the combination of fat and PRP in the context of facial lipostructure surgery30.
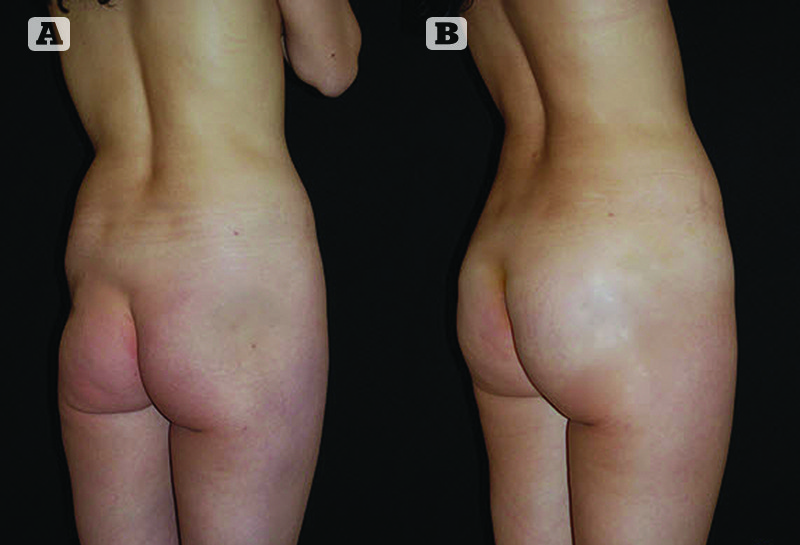
Figure 5 (A) Preoperative photos of a 40-year-old woman requesting gluteal correction after trauma, and (B) postoperative photos after gluteal augmentation by stromal enriched lipograft
An important consideration for harvesting and refinement in preparation for grafting is to respect and maintain the tissue architecture of living fat31. Any mechanical or chemical insult that damages the fragile tissue architecture of fat will result in eventual necrosis of the injected fat32. Even when large areas need reconstruction, like in head and neck cancers, it is possible to use the SEL technique as a tissue engineering method of reconstruction. The SEL technique also offers the possibility of prefabrication of flaps, reconstruction of auricular framework defects, and fabrication of new skin for massive burns when SVF is used either alone or combined with other natural or synthetic biomaterials. Successful SEL graft requires attention to patient preparation, meticulous planning, and optimising the harvesting, storage, and transplantation of adipose tissue. SEL is a living tissue that must be in close proximity to a nutritional and respiratory source to survive33. In aesthetic plastic surgery, the SEL technique provides a safer alternative to allogenic implant use, resulting in the creation of a functional tissue which has a more natural look and carries fewer risks than currently available augmentation options. The SEL graft achieves cell based therapy within a single surgical procedure, thereby avoiding lengthy and costly in vitro culturing steps. The apparent commercial and industrial interest on SEL that has emerged lately has encouraged the scientific community in scheduling new clinical trials34. A number of companies (e.g. Cytori Therapeutics, Inc., Medikan International, Inc., Sceldis) have launched medical systems based on the principle of isolating stromal vascular fraction that are applied in clinical trials in the fields of urology, cardiac surgery, neurology and plastic surgery.
Conclusions
There is a wealth of published clinical data showing safety, feasibility, and efficacy of the SEL technique. The current applications and the future perspectives of adipose tissue engineering unquestionably represent innovative techniques with huge therapeutic potential that must be balanced against the stringent standards of scientific and clinical investigation.

